
Download

ORIGINAL ARTICLE
From triggers to treatment: An epidemiological exploration of anaphylaxis in a lower middle-income area in Colombia
Yorlady Muñoza, Tomas Roseroa, Sofia Martínez Betancurb, Jacobo Triviño Ariasb*, Oriana Arias-Valderramaa,b, Jessica Largo Ocampoa, Carlos Daniel Serranoa,c, Manuela Olayaa,c
aUniversidad ICESI, Facultad de Ciencias de la Salud, Departamento de Medicina, Cali, Colombia
bCentro de Investigaciones Clínicas, Fundación Valle del Lili, Cali, Colombia
cServicio de Alergología, Fundación Valle del Lili, Cali, Colombia
Abstract
In this cross-sectional, descriptive, and observational study conducted at Fundación Valle del Lili in Colombia, the clinical and sociodemographic characteristics of anaphylaxis were investigated in a cohort of 80 patients who sought medical care between January 2021 and December 2022. With a median age of 16 years and a notable prevalence among individuals aged below 18 years, the study revealed that 63.8% of patients had concomitant allergic diseases. Medications emerged as the primary triggers for anaphylaxis, followed by food. The mucocutaneous system was predominantly affected in 55% of cases, with respiratory involvement observed in 37.5%. Alarmingly, anaphylactic shock occurred in 17.5%, and 7.5% experienced biphasic anaphylaxis. Intramuscular adrenaline was administered in 88.8% of cases, with 75% of patients not receiving an allergy consultation upon discharge, and 52.5% lacking follow-up for allergy care. Considering that in Colombia epidemiological data on the clinical and sociodemographic aspects of anaphylaxis remain largely unknown, this study documents the features of anaphylaxis in both adult and pediatric populations and highlights the urgent need for improved awareness, timely evaluation by allergists, and comprehensive follow-up care for individuals experiencing anaphylaxis.
Key words: Anaphylaxis, characterization, adults, pediatrics, allergen, adrenaline
*Corresponding author: Jacobo Triviño Arias, Fundación Valle del Lili, Cra 98 N°18-49, Cali, Colombia. Email address: [email protected]
Received 6 May 2024; Accepted 7 August 2024; Available online 1 September 2024
Copyright: Muñoz Y, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Anaphylaxis is a life-threatening systemic hypersensitivity reaction that manifests as a rapid-onset response to various triggering agents, often characterized by systemic mast cell degranulation.1,2 It involves at least two systems, including mucocutaneous, respiratory, gastrointestinal, cardiovascular, and central nervous systems.1–3 Anaphylaxis is a significant reason for both adult and pediatric patients to seek medical attention.4
Globally, the estimated annual incidence of anaphylaxis ranges from 1.5 to 7.9 cases per 100,000 people in the general population, with higher rates in the pediatric population. The incidence is highest in children aged between 0 and 4 years.5,6 In many Latin American countries, including Colombia, the epidemiological profile of anaphylaxis is limited. According to the Latin American Anaphylaxis Registry, the median age for anaphylaxis is 26 years, with a high predominance in the female population in the cases of adult and elderly patients.3 The pediatric population mainly comprised male patients, with more frequency in patients with a history of atopy, mainly those with atopic dermatitis.3
Mortality due to anaphylaxis is generally low. Annually, a rate of 0.05–0.51 per 1,000,000 people is attributed to medications, 0.03–0.32 to food, and 0.09–0.13 is linked to hymenoptera exposure. The clinical presentation evolves swiftly. Without prompt treatment, it can be potentially fatal due to its multisystem involvement. Early recognition of anaphylactic symptoms is important to prevent fatal outcomes.7,8
The objective of this study was to document the clinical and sociodemographic features of anaphylaxis in both adult and pediatric populations who sought medical care in a high-complexity hospital in Colombia, between January 2021 and December 2022.
Methods
Area of study
This study was performed at a reference center for critical care in southwest Colombia, which provides high-quality treatment equipment, medications, and diagnostic aids.
Variables
We collected variables from clinical records related to demographic data, triggers, clinical presentation, and treatment.
Patients with a sudden reaction of hypersensitivity with compromise of the respiratory system, with skin involvement, with or without circulatory shock, with an exposure to any allergen, and those who met the criteria proposed by the Galaxy guideline were included in the study. Patients could be in the emergency room (ER) or another location in the hospital. The patients who were administered intramuscular adrenaline were identified in order to enhance the detection of patients diagnosed with anaphylaxis.
Patients experiencing acute onset reactions not meeting the diagnosis clinical criteria for anaphylaxis, those with symptoms indicative of drug or toxic poisoning related with adverse effects without hypersensitivity, and individuals exhibiting allergic nonanaphylactic reactions were excluded from the study.
Statistical Analysis
The descriptive analysis of demographic characteristics was conducted by assessing the distribution of quantitative variables using the Shapiro–Wilk test. The results are presented as either median with interquartile range or mean with standard deviation, depending on the data distribution. The exact Fisher test was used to evaluate differences between groups in qualitative variables. All the analyses were performed with R Studio software version 4.3.3.
The study adhered to the prevailing regulations governing bioethical research and received approval (Approval Number: 02063) from the institution’s ethics committee, specifically the Biomedical Research Ethics Committee of the Fundación Valle del Lili´s IRB. Given the study design, obtaining informed consent was deemed unnecessary.
Results
The study comprised 80 patients; 42 (52.5%) of them were male, and 41 patients (51.2%) were aged below 18 years. The predominant setting for patient presentations was the emergency department, accounting for 87.5%, followed by hospitalization wards (10%), the intensive care unit (ICU) (1.3%), and outpatient clinics (1.3%). Twelve patients (15%) had at least one previous episode of anaphylaxis, 22 (27.5%) had drug allergies, 9 (11.2%) had allergic rhinitis, 8 (8.8%) had asthma, and eight (8.8%) had food allergies. Of all the patients, 28 (35%) had associated comorbidities. Of those, 12 (42.9%) had a history of cardiovascular disease, and 6 (21.4%) had concurrent infections. Other disease data are the following: one each with neurological and kidney diseases (3.6%), and four each with rheumatological and oncological ailments (14.3%) Table 1.
Table 1 Demographic data.
| Variable | N = 80a |
|---|---|
| Gender | |
| Woman | 38 (47.5%) |
| Man | 42 (52.5%) |
| Age | 16.0 (9.0, 37.0) |
| Categorical age | |
| <18 years | 41 (51.2%) |
| ≥18 years | 39 (48.8%) |
| Allergic disease | |
| No history | 29 (36.2%) |
| Allergic rhinitis | 9 (11.2%) |
| Allergic asthma | 7 (8.8%) |
| Urticaria | 3 (3.8%) |
| Atopic dermatitis | 2 (2.5%) |
| Food allergy | 8 (10.0%) |
| Drug allergy | 22 (27.5%) |
| Hymenoptera Allergy | 0 (0.0%) |
an (%); Median (IQR)
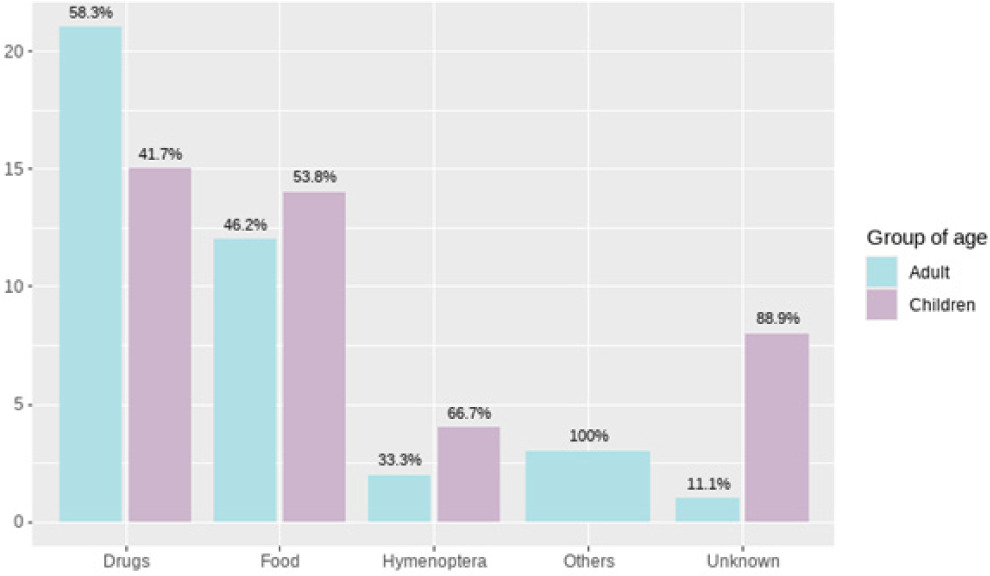
The clinical characteristics of anaphylaxis between adults and children show a statistical difference of p=0.031 related to the trigger. Drugs were the most common cause among adults, while in children, foods and drugs had the same incidence rate (Table 2 and Figure 1).
Table 2 Clinical features of anaphylaxis.
| Variable | Adults N=39a | Children N=41 | P-valueb |
|---|---|---|---|
| Suspected allergen | |||
| Unknown | 1 (2.6%) | 8 (19.5%) | 0.031 |
| Food | 12 (30.8%) | 14 (34.1%) | |
| Drugs | 21 (53.8%) | 15 (36.6%) | |
| Hemiptera | 2 (5.1%) | 4 (9.8%) | |
| Others | 3 (7.7%) | 0 (0.0%) | |
| Food allergen | |||
| Eggs | 0 (0.0%) | 1 (7.1%) | 0.001 |
| Peanut | 1 (8.3%) | 1 (7.1%) | |
| Seafood | 7 (58.3%) | 0 (0.0%) | |
| Cow milk | 0 (0.0%) | 4 (28.6%) | |
| Fruits | 0 (0.0%) | 1 (7.1%) | |
| Gluten | 1 (8.3%) | 0 (0.0%) | |
| Others | 3 (25.0%) | 7 (50.0%) | |
| System involvement | |||
| Mucocutaneous | 19 (48.7%) | 25 (61.0%) | 0.5 |
| Cardiovascular | 2 (5.1%) | 3 (7.3%) | |
| Respiratory | 17 (43.6%) | 13 (31.7%) | |
| Gastrointestinal | 1 (2.6%) | 0 (0.0%) | |
| Neurologic | 0 (0.0%) | 0 (0.0%) | |
| Anaphylactic shock | 10 (25.6%) | 4 (9.8%) | 0.062 |
| Grade of reaction | |||
| Grade 1 | 2 (5.1%) | 1 (2.4%) | 0.017 |
| Grade 2 | 3 (7.7%) | 15 (36.6%) | |
| Grade 3 | 8 (20.5%) | 9 (22.0%) | |
| Grade 4 | 17 (43.6%) | 9 (22.0%) | |
| Grade 5 | 9 (23.1%) | 7 (17.1%) |
an (%); Median (IQR); bFisher’s exact test
Figure 1 Anaphylaxis trigger by age group.
Drug-induced anaphylaxis was reported only in 36 patients, the most common being NSAIDs and antibiotics. Regarding food-induced anaphylaxis, seafood was most frequently involved.
The mucocutaneous system was affected in 61% of children, whereas it was the respiratory system in 43.6% of adults.
The grading of anaphylaxis severity revealed that 22 (27.5%) patients had a mild reaction, 43 (53.8%) had a moderate reaction, and 15 (18.8%) had a severe reaction. Regarding the grade of reactions, the distribution showed that grade 4 reactions were the most common in 26 (32.5%) patients, followed by grade 2 in 18 (22.5%) patients, grade 3 in 17 (21.2%) patients, and grade 5 in 16 (20%) patients, with a statistical difference of p=0.017 among adults and children.
Out of the observed cases, 14 (17.5%) patients presented with anaphylactic shock, while 6 patients (7.5%) displayed biphasic anaphylaxis. The assessment of serum tryptase levels was conducted only in 10 patients (12.5%), revealing that 70% of these individuals had concentrations below 11.4 ng/mL.
Adrenaline was administered to all patients, predominantly through intramuscular injection in 71 cases (88.8%). The intravenous (IV) mode was used in 4 (5.0%) patients, and the subcutaneous mode was used in 5 (6.2%) patients. Additional supportive measures, including the use of IV fluids, were implemented in 33 cases (41.2%), and supplemental oxygen therapy was employed in 32 (40%) cases. Utilization of other drugs was widespread, with glucocorticoids being administered in 61 (76.2%) of cases, followed by antihistamines in 50 (62.5%) cases and salbutamol in 21 (26.2%) cases. On the other hand, inotropic or vasoactive support was limited to 5 cases (6.2%) (Figure 2).
Figure 2 Treatment of anaphylaxis.
Fifty-one patients (63.7%) underwent observation in the ER, 10 patients (12. 5%) were attended in the ER and discharged, 13 patients (16.2%) were admitted to the ICU, and 6 patients (7.5%) needed hospitalization. In terms of inpatient management duration, 59 (73.8%) stayed less than 24 hours, while 15 (18.8%) stayed at least 48 hours.
A total of 60 patients received a prescription at the time of discharge. Among these, 25 (31.2%) had prescriptions for glucocorticoids and 46 (57.2%) for antihistamines. Intrahospital allergology consultations were carried out in 9 patients (11.2%). Outpatient follow-up by allergology occurred in 32 patients (40%).
Discussion
Anaphylaxis remains a significant challenge in clinical settings.1,2 Despite its low mortality rate, anaphylaxis continues to be a substantial cause of hospitalization, particularly among pediatric patients.1 In our study, we had 80 patients. We did not find a significant gender difference in patients with anaphylaxis, although there was a slight male predominance. A modest proportion of patients belonged to the pediatric population (51.25%), with a mean age of 16 years. This contrast with the global literature where a higher incidence in pediatric patients, particularly elevated during the first 2 years of life, is described.5
Most patients had a past medical history, particularly cardiovascular diseases in the adult population. However, we found patients with oncological and rheumatological conditions, which may be because we are a reference center in our region for high-complexity diseases. A remarkable observation was the high percentage of drug-induced anaphylaxis. This finding contrasts with several studies, including the Latin American Registry,9 which reported a higher prevalence of food as a trigger for anaphylaxis. This may be again secondary to being a reference center for high-complexity diseases.
The main drugs we found to induce anaphylaxis in our study were NSAIDs, a finding consistent with global data. However, this contrasts with the Latin American Registry,9 which reported a higher incidence of antibiotics as the causal agent. Food allergies demonstrated a predictable pattern, with dairy products and seafood emerging as significant causes of anaphylactic reactions.9,10 However, in global literature, there is a predominance of nuts, milk, and eggs.1
Our study also utilized the primary affected system variable to identify the first manifestation; more than 50% of the patients exhibited mucocutaneous compromise. This includes reactions such as urticaria or angioedema, aligning with findings in some studies,9,12 where most cases primarily presented with mucocutaneous reactions. There was a significant presentation of respiratory symptoms that could be associated with chronic respiratory conditions such as asthma. The cardiovascular system was part of severe reactions such as anaphylactic shock, accounting for 17.5% of cases. Therefore, it is crucial for clinicians to rapidly identify severe anaphylaxis and administer appropriate treatment.1,11,12
The temporal aspect of anaphylaxis presentation emerges as a pivotal consideration in our study, revealing a significant prevalence of cases with indeterminate timing. This may cause a delay in the diagnosis and early treatment. The infrequent utilization of serum tryptase in our study, despite its recognized efficacy in discerning biphasic anaphylaxis and aiding in the identification itself, is noteworthy.1,2 This tendency is congruent with findings in the Latin American registry, elucidating the lack of data on this biomarker, probably due to its limited availability in Latin America.9 Importantly, our institution has accessible serum tryptase, yet clinical practice considerations emerged as the primary determinant in its infrequent usage. Instances where serum tryptase was employed included cases of ambiguous anaphylaxis within the ICU or hospitalization settings.
Biphasic anaphylactic reactions occurred in 7.5% of the patients; this incidence is notably higher than that reported in a Japanese study,13 where it constituted 1.7% of cases. On the other hand, across various registries, the prevalence of biphasic anaphylaxis was in a range of 0.9% to 14.7%, thereby placing our collected data within this established spectrum.1
The treatment of anaphylaxis is clearly outlined in the guidelines provided by the Spanish Society (Galaxy 2016 and 2022) and the European Academy of Allergy and Clinical Immunology (EAACI), supporting intramuscular adrenaline as the primary therapeutic approach.1,2,9,11 In our study, in 88.8% of the cases, intramuscular adrenaline was administered as per the guidelines. However, the use of intramuscular adrenaline varies considerably across different studies; for instance, a study in Thailand reported near universal use,11 whereas the Latin American registry documented a lower rate of 43%.9 The above highlights the critical need for targeted training initiatives and the implementation of guidelines to ensure the universal correct use of adrenaline in anaphylaxis management.
The pharmacological management of anaphylactic reactions in our institution reveals widespread use of glucocorticoids, coinciding with registries that emphasize the significant role of glucocorticoids in anaphylaxis management.9,12,14 While clinical practice guidelines recommend the use of corticoids in anaphylaxis, they emphasize that they should not be considered as the first-line treatment. The administration of steroids is often associated with moderate to severe reactions, particularly in conjunction with the use of adrenaline, and is frequently employed in suspected biphasic reactions. In our study, a similarly high percentage of cases involved systemic antihistaminic drugs and bronchodilators. The outcomes of anaphylaxis underline that most patients in our institution had relatively short stay times, typically less than 24 hours, primarily within the observation unit. Hospitalizations and ICU admissions were infrequent.
Despite all patients having prescriptions upon discharge, none of them received adrenaline as a first-line outpatient medication; instead, all of them had prescribed systemic corticosteroids and antihistamines, contrary to international guidelines.10,15
Moreover, intrahospital consultations with allergology were notably infrequent, underscoring the significance of adhering to the recommended follow-up by allergology, a practice not universally adopted as advocated by established guidelines.1,2 Nearly half of the patients advised for follow-ups did not avail the institutional allergology services. They were influenced by biases related to those observed in other healthcare institutions or because healthcare providers due to administrative actions did not authorize their follow-up in our institution. Consequently, the imperative arises, both in pediatric and adult populations, to endorse allergology follow-ups. Comprehensible -follow-ups are indispensable for discerning the real cause of anaphylaxis and establishing an effective treatment regimen.
Limitations
The limitation of this study lies in being a retrospective study with a review of medical records with allergic diseases in CIE-10 and adrenaline use. This may leave many events out of scope.
Conclusion
Our study highlights a significant reality within our institution. Despite low levels of mortality observed in anaphylactic patients, there is still a substantial challenge for improvement in achieving optimal anaphylaxis management. Areas for improvement include the identification of anaphylactic triggers, the universal use of intramuscular adrenaline, and ensuring consistent follow-ups with allergology. These aspects represent crucial facets requiring improvement to align with established guideline recommendations.1,2 While our institution demonstrates more positive rates in several correct clinical practices compared to the region,9 there remains a pressing need for overall improvement in the approach toward anaphylaxis. The findings also prompt reflection on how anaphylaxis is managed in high-complexity centers in Latin America, emphasizing the limited translation of practices into general clinical settings. It is imperative to generate more robust and comprehensive data on anaphylaxis, to facilitate the implementation of enhanced practices, ultimately fostering positive outcomes for patients with anaphylactic reactions in both the short and long term.
Conflict of interest
The authors state no conflict of interest.
Acknowledgements
The authors thank Dr. Juan P. Díaz-Solórzano for language editing to improve the quality of the manuscript.
Funding
This project was funded by “Fundación Valle del Lili”. Funder grant number is not Applicable.
REFERENCES
1. Muraro A, Worm M, Alviani C, Cardona V, DunnGalvin A, Garvey LH, et al. EAACI guidelines: Anaphylaxis (2021 update). Allergy. 2022;77(2):357–77. 10.1111/all.15032
2. Cardona V, Cabañes N, Chivato T, De La Hoz B, Fernández M, et al. Guía de actuación en ANAFILAXIA: GALAXIA 2016. Sociedad Española de Alergología e Inmunología Clínica (SEAIC) 2016; 19130(2016):1–18.
3. Cardona V, Álvarez-Perea A, Ansotegui-Zubeldia I, Arias-Cruz A, Ivancevich J, González-Díaz S, et al. Guía de Actuación en Anafilaxia en Latinoamérica. Galaxia-Latam. Rev Alerg Mex. 2019; 66(6):1–39. 10.29262/ram.v66i6.588
4. Poowuttikul P, Seth D. Anaphylaxis in Children and Adolescents. Pediatr Clin North Am. 2019;10(01):995–1005. 10.1016/j.pcl.2019.06.005
5. Tanno L, Bierrenbach AL, Simons F, Cardona V, Thong BYH, Molinari N, et al. Critical view of anaphylaxis epidemiology: Open questions and new perspectives. AACI. 2018; 14(1):2. 10.1186/s13223-018-0234-0
6. Cardona V, Chivato T, Diéguez M, Escudero C, Fernández Menéndez V, Fernández Rivas M, et al. Guía de actuación en anafilaxia: GALAXIA 2022. Sociedad Española de Alergología e Inmunología Clínica (SEAIC). 2022; 33(6):474–487. 10.18176/19264-19-0
7. McLendon K, Sternard BT. Anaphylaxis. StatPearls (content is king). Last update: 2023 January 26.
8. Londoño J, Raigosa M, Vásquez M, Sánchez J. Anaphylaxis: State of the art. Iatreia. 2018;31(2):166–79. 10.17533/udea.iatreia.v31n2a05
9. Jares EJ, Cardona V, Gómez RM, Bernstein JA, Rosario Filho NA, Cherrez-Ojeda I, et al. Latin American anaphylaxis registry. World Allergy Organ J. 2023; 16(2):100748. 10.1016/j.waojou.2023.100748
10. de Silva D, Singh C, Muraro A, Worm M, Alviani C, Cardona V, DunnGlvin A, et al. Diagnosing, managing and preventing anaphylaxis: Systematic review. Allergy: European Journal of Allergy and Clinical Immunology. 2021;76(5):1493–506. 10.1111/all.14580
11. Long B, Gottlieb M. Emergency medicine updates: Anaphylaxis. Am J Emerg Med. 2021; 49:35–9. 10.1016/j.ajem.2021.05.006
12. Uppala R, Phungoen P, Mairiang D, Chaiyarit J, Techasatian L. Pediatric anaphylaxis: Etiology and predictive factors in an emergency setting. Glob Pediatric Health. 2021; 8:2333794X2110113. 10.1177/2333794X211011301
13. Ikegawa K, Morikawa E, Nigo A, Hataya H, Akasawa A. Epidemiology of anaphylaxis and biphasic reaction in Japanese children. Acute Med Surg. 2021; 8(1):e688. 10.1002/ams2.688
14. Liyanage CK, Galappatthy P, Seneviratne SL. Corticosteroids in management of anaphylaxis; a systematic review of evidence. Eur Ann Allergy Clin Immunol. 2017; 49(05):196. 10.23822/EurAnnACI.1764-1489
15. Dibrin TE, Wasserman S, Turner PJ. Who needs Epineprhine? Anaphylaxis autoinjectors and parachutes. J Allergy Clin Immunol Pract. 2023; 11(4):1036–46. 10.1016/j.jaip.2023.02.002