
Download
ORIGINAL ARTICLE
Analysis of the diagnostic value of coagulation markers and coagulation function indices on the occurrence of DIC in sepsis and its prognosis
Xiaowei Fang, Wei Fu*, Luyang Xu, Yichao Qiu
Department of Emergency, The Second Affiliated Hospital, Jiangxi Medical College, Nanchang University, Nanchang Jiangxi Province, China
Abstract
Sepsis is a life-threatening condition that has the potential to multiple organ dysfunction and mortality. One of its frequent complications is disseminated intravascular coagulation (DIC), characterized by hyperactive clotting mechanisms that cause widespread clot formation and tissue damage. This study aimed to investigate early diagnostic markers of sepsis-associated DIC by comparing inflammatory factor levels, 28-day survival rates, coagulation function, and markers between patients with sepsis (non-DIC group) and those with sepsis-induced DIC (DIC group). The study analyzed the diagnostic efficacy of coagulation function and markers in predicting the occurrence and prognosis of sepsis-associated DIC, presenting survival curves. Results indicated significantly increased levels of APTT, TAT, tPAIC, PIC, and sTM in the DIC group compared to the non-DIC group. Sequential Organ Failure Assessment (SOFA) scores on days 1, 3, and 7 were notably lower in the non-DIC group. Correlation analysis revealed positive associations between PT, APTT, TAT, tPAIC, PIC, sTM levels, and SOFA scores, as well as negative associations with Fib and SOFA scores. Survival curves showed substantially lower mortality rates in the non-DIC group, highlighting significant survival disparities between groups. Combining all four coagulation indicators (TAT+ tPAIC + PIC + sTM) showed promising diagnostic value in evaluating disease severity, early DIC diagnosis, and sepsis prognosis.
Key words: sepsis, coagulation markers, coagulation indicators, diagnostic value, DIC, prognosis
*Corresponding author: Wei Fu, Department of Emergency, The Second Affiliated Hospital, Jiangxi Medical College, Nanchang University, No. 1 Minde Road, Donghu District, Nanchang City, Jiangxi Province, 330000, China. Email address: [email protected]
Received 28 April 2024; Accepted 4 July 2024; Available online 1 September 2024
Copyright: Fang X, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Sepsis is a life-threatening condition caused by the dysregulated systemic response to infection, resulting in organ dysfunction and substantial morbidity and mortality rates.1 Global hospital data indicate annual incidence of 189 cases per 100,000 individuals, highlighting sepsis as a significant public health issue.2 Previous studies have considered coagulation disorders as a complication that arises in the later stages of sepsis. However, recent domestic and international animal experiments and clinical studies have increasingly shown that coagulation abnormalities are present throughout the entire pathological progression of sepsis. These findings highlight coagulation dysfunction as a critical factor that affects both the onset and prognosis of sepsis.3,4 The pathogenesis of coagulation disorders in sepsis includes overproduction of thrombin, reduction of endogenous anticoagulant substances, and inhibition of fibrinolysis, leading to the development of microvascular thrombosis, which may progress to disseminated intravascular coagulation (DIC) in severe cases.5 DIC is a challenging syndrome in the field of critical care, and it is relatively difficult to diagnose clinically. Previous studies have established a clear correlation between the existence of DIC in sepsis and the severity and prognosis of the illness. It has been confirmed that the presence and absence of DIC in sepsis is closely correlates with the severity and prognosis of the disease, and the morbidity and mortality rates are significantly higher in patients with apparent DIC compared to those without apparent DIC.6 Therefore, timely identification and intervention of sepsis-induced DIC play a critical role in improving outcomes. Early diagnosis of DIC in sepsis has been challenging because DIC diagnostic scoring indices focus on coagulation factor and platelet deficiencies, which are typically observed in the later stages of DIC.7 It has been found that more sensitive coagulation markers for coagulation or fibrinolytic activation are likely to be useful for early diagnosis of DIC.8 Earlier studies have confirmed that markers such as thrombin-antithrombin complex (TAT) and plasminogen antifibrinolytic complex (PIC) show a notable increase before and after the diagnosis of DIC. However, they are not necessarily associated with multiple organ failure or prognosis.9 Tissue plasminogen activator inhibitor complex (t-PAIC) and soluble thrombomodulin (sTM) were found to be significantly elevated both before and after the diagnosis of DIC, but these markers were not associated with multi-organ failure or prognosis.10 Previous studies have confirmed that the coagulation markers mentioned above have a certain diagnostic value for DIC. However, the primary focus of these studies has been on individuals with hematologic and solid tumors, with limited research specifically on patients with sepsis.11,12 For this reason, the following study was conducted to explore the early diagnostic value of markers of coagulation and cellular damage in predicting the prognosis of sepsis-associated DIC.
Information and Methods
General information
A retrospective study was conducted at the emergency intensive care unit and central care unit of The Second Affiliated Hospital, Jiangxi Medical College. The study included patients diagnosed with sepsis upon admission from January 2022 to January 2023.
Inclusion criteria of the study: age ≥ 18 years; diagnosis of sepsisaccording to the Sepsis-3.0 diagnostic criteria;13 all enrolled patients had complete clinical data available, and voluntarily signed an informed consent form.
Exclusion criteria of the study: history of hematologic disorders; previous coagulation system-related disorders such as heparin-induced thrombocytopenia and thrombotic thrombocytopenic purpura; patients with concomitant malignancies; antiphospholipid syndrome; trauma, intoxication, or pregnancy; cirrhosis Child-Pugh class C; history of thrombophilia disorders (antithrombin deficiency, protein S deficiency, and protein C deficiency); and patients who had received anticoagulant medication (warfarin, dabigatran, rivaroxaban, and heparin/low molecular heparin) prior to enrollment; incomplete clinical data; psychiatric or other illnesses leading to very poor compliance; reluctance to participate in the study and failure to provide a signature on the informed consent form.
The Ethics Committee of our hospital approved the study protocol and grantedpermission for the study to be conducted.
Data collection
Collection of basic data of patients at subgroup level
A total of 100 patients were divided into two groups: the DIC group, which consisted of 34 patients diagnosed according to the diagnostic criteria of the International Society on Thrombosis and Haemostasis (ISTH), and the non-DIC group, which included 66 patients. The study recorded and analyzed the age, gender, site of infection, and underlying diseases of patients in both groups.
Research methods and index observation
All patients received anti-infective treatment and fluid resuscitation according to the 2016 “Save the Sepsis Campaign” (SSC) guidelines.14 Vasoactive drugs and mechanical ventilation were admistered as needed to support respiration, along with symptomatic supportive treatment for various organ systems.
Upon admission, the index information was collected, including serum levels of cytokines [Tumor necrosis -factor-α (TNF-α), C-reactive protein (CRP), interleukin 6 (IL-6)], coagulation function tests [prothrombin time (PT), activated partial thromboplastin time (APTT), and fibrinogen (Fib)]. In addition, coagulation markers [Thrombin-antithrombincomplex (TAT), t-PAIC, plasmin antiplasmin complex (PIC), and soluble thrombomodulin (sTM)] were measured.
TNF-α and IL-6 were detected using enzyme-linked immunosorbent assay, while CRP was measured by immunoturbidimetric assay. Coagulation function was assessed using an ACL TOP 700 automatic coagulation analyzer from Wolfen, USA. The four coagulation markers were detected using a “Shine I automatic luminescence immunoassay analyzer” from Shenzhen Yingkai. The detection kits were purchased from Wuhan Jilide Biotechnology Co., Ltd. (East Lake New Technology Development Zone, Wuhan, Hubei Province, China).
A chemiluminescence enzyme immunoassay was used as the detection method.
Assessment of disease severity indicators
The corrected Acute Physiology and Chronic Health Evaluation II (APACHE II)15 and the corrected Sequential Organ Failure Assessment (SOFA) score16 were assessed at three time points: on day 1, day 3, and day 7.
Secondary endpoint indicators
The 28-day survival of patients in the two groups was recorded, and survival curves were plotted to analyze and compare the outcomes between the DIC and non-DIC groups.
Statistical methods
The study data were analyzed using SPSS 23.0 software. Measurement data were described statistically as (X ± SD). Count data that followed a normal distribution were analyzed using the chi-square test, while data that did not follow a normal distribution were expressed as median values (25%, 75%) and analyzed using the Mann-Whitney U test. To examine the correlation between coagulation markers, cytokines, and patient prognosis, Spearman’s rank correlation coefficient was employed. The absolute value of correlation coefficient above 0.7 indicated strong correlation, the absolute value of correlation coefficient between 0.3 and 0.7 was moderate correlation, and the absolute value of correlation coefficient below 0.3 was considered as weak correlation or irrelevant. Receiver Operating Characteristic (ROC) curves were plotted, and the area under the curve (AUC) was calculated to assess the diagnostic accuracy of study variables for predicting the occurrence of DIC and death. Finally, survival curves for 28 days survival were analyzed using the Kaplan-Meier method. A significance level of p<0.05 indicated that differences between groups were statistically significant.
Results
Comparison of the results of the general information of the two groups of patients
The study found that among 100 sepsis patients, 34% developed DIC. The comparison of age, sex ratio, site of infection, underlying disease, and serologic indices between the two groups was not statistically significant (p>0.05). However, there were significant differences in the levels of platelets and WBC between the DIC group and the non-DIC group (p<0.05). The results are shown in Table 1.
Table 1 Comparison of general information and levels of inflammatory factors between the two groups of patients.
| Information | DIC group (n=34) | Non-DIC group (n=66) | χ2/t | p |
|---|---|---|---|---|
| Average age (yrs) | 61.87±8.48 | 59.23±9.87 | 1.325 | 0.188 |
| Male-to-female sex ratio | 19/15 | 42/24 | 0.567 | 0.451 |
| Site of infection | 0.484 | 0.922 | ||
| Respiratory system | 11 | 21 | ||
| Digestive system | 13 | 25 | ||
| Urinary system | 9 | 16 | ||
| Other sites | 1 | 4 | ||
| Underlying diseases | 0.175 | 0.916 | ||
| Hypertension | 16 | 29 | ||
| Coronary heart disease | 6 | 11 | ||
| Diabetes | 9 | 20 | ||
| TNF-α(pg/mL) | 89.57±11.50 | 88.04±12.85 | 0.584 | 0.561 |
| CRP(mg/L) | 130.13±40.84 | 120.24±33.63 | 1.293 | 0.199 |
| IL-6(pg/mL) | 191.34±47.46 | 188.47±52.21 | 0.268 | 0.789 |
| WBC(*109/L) | 23.72±4.94 | 17.37±3.30 | 7.656 | <0.001 |
| Platelets(*1012/L) | 59.52±17.61 | 171.92±49.57 | 12.786 | <0.001 |
Comparison of coagulation function indexes of patients in two groups
The results of the coagulation function indices of the two groups of patients on day 1, day 3, and day 7 are shown in Table 2. There was no significant difference between the two groups of patients except for the comparison of PT indices detected on day 3 and day 7 (p>0.05). Compared to the DIC group, patients in the non-DIC group had significantly lower PT on day 1, APTT on days 1, 3, and 7, and significantly higher Fib on days 1, 3, and 7 (p<0.05).
Table 2 Comparison of coagulation function indices of patients in the two groups.
| Indicators | DIC group (n=34) | Non-DIC group (n=66) | t | p | |
|---|---|---|---|---|---|
| PT(s) | Day 1 | 18.17±3.03 | 16.13±2.84 | 3.325 | 0.001 |
| Day 3 | 16.68±2.55 | 16.55±2.46 | 0.243 | 0.809 | |
| Day 7 | 15.83±2.60 | 14.87±2.46 | 1.785 | 0.077 | |
| APTT(s) | Day 1 | 53.25±7.34 | 40.81±6.94 | 8.324 | <0.001 |
| Day 3 | 47.17±6.08 | 36.21±6.55 | 8.115 | <0.001 | |
| Day 7 | 42.19±9.33 | 35.39±5.09 | 4.725 | <0.001 | |
| Fib(g/L) | Day 1 | 3.56±1.04 | 4.91±1.99 | 3.670 | <0.001 |
| Day 3 | 3.53±0.92 | 4.99±1.01 | 7.041 | <0.001 | |
| Day 7 | 3.19±0.73 | 4.26±1.02 | 5.425 | <0.001 | |
Comparison of coagulation marker levels between the two groups of patients
The results of coagulation markers of patients in the two groups on day 1, day 3, and day 7 are shown in Table 3. Compared to the DIC group, the levels of TAT, tPAIC, PIC, and sTM indices of patients in the non-DIC group were significantly lower (p<0.05).
Table 3 Comparison of coagulation marker levels between the two groups of patients
| Indicators | DIC group (n=34) | Non-DIC group (n=66) | t | p | |
|---|---|---|---|---|---|
| TAT (ng/mL) |
Day 1 | 14.90±1.37 | 10.26±3.64 | 7.157 | <0.001 |
| Day 3 | 12.03±2.21 | 6.18±1.98 | 13.468 | <0.001 | |
| Day 7 | 10.37±1.18 | 6.11±2.10 | 10.977 | <0.001 | |
| tPAIC (ng/mL) |
Day 1 | 29.17±8.78 | 16.24±4.63 | 9.668 | <0.001 |
| Day 3 | 31.21±8.07 | 12.16±3.76 | 16.128 | <0.001 | |
| Day 7 | 32.69±8.27 | 9.77±3.16 | 19.938 | <0.001 | |
| PIC (µg/mL) |
Day 1 | 3.25±0.84 | 1.70±0.56 | 11.030 | <0.001 |
| Day 3 | 2.85±0.74 | 1.13±0.40 | 15.116 | <0.001 | |
| Day 7 | 2.55±0.52 | 0.82±0.24 | 22.531 | <0.001 | |
| sTM (U/mL) |
Day 1 | 30.89±11.68 | 18.97±7.13 | 6.323 | <0.001 |
| Day 3 | 30.20±9.34 | 15.62±4.73 | 10.378 | <0.001 | |
| Day 7 | 25.37±11.59 | 12.29±3.57 | 8.456 | <0.001 | |
Comparison of disease severity indicators between the two groups
The statistical values of SOFA scores along with APACHE II scores of patients in the two groups at different times are shown in Table 4. It can be seen that compared to the DIC group, SOFA scores were significantly lower in the non-DIC group on days 1, 3, and 7 (p<0.05). APACHE II scores were significantly lower in the non-DIC group compared to the DIC group on day 7. On days 1 and 3, although there was a trend towards lower APACHE II scores in the non-DIC group, the difference did not reach statistical significance (p<0.05).
Table 4 Comparison of disease severity indicators between the two groups.
| Indicators | DIC group (n=34) | Non-DIC roup (n=66) | t | p | |
|---|---|---|---|---|---|
| SOFA score | Day 1 | 10.95 (7.94,15.40) | 5.63 (4.05,6.42) | 6.617 | <0.001 |
| Day 3 | 8.79 (6.98,10.13) | 4.53 (3.70,5.53) | 6.192 | <0.001 | |
| Day 7 | 7.15 (5.82,8.68) | 2.11 (1.68,2.53) | 6.982 | <0.001 | |
| APACHE II score | Day 1 | 16.32±6.73 | 15.33±4.82 | 0.844 | 0.401 |
| Day 3 | 15.77±8.23 | 13.62±4.24 | 1.729 | 0.087 | |
| Day 7 | 14.69±4.12 | 11.69±3.44 | 3.857 | 0.000 | |
These findings suggest that patients in the non-DIC group had lower severity scores (SOFA and APACHE II) compared to those in the DIC group.
Correlation analysis
The results of the correlation of coagulation function as well as coagulation markers with the scores of disease severity are shown in Table 5. The results of correlation analysis showed that patients' PT, APTT, TAT, tPAIC, PIC, and sTM were significantly and positively correlated with patients' SOFA scores, whereas Fib was significantly and negatively correlated with SOFA scores (p<0.05). APACHE II score did not correlate with the level of the above indicators (p>0.05).
Table 5 Correlation analysis.
| Indicators | SOFA score | APACHE II score | ||
|---|---|---|---|---|
| r | p | r | p | |
| PT | 0.272 | 0.006 | 0.083 | 0.413 |
| APTT | 0.458 | 0.000 | 0.024 | 0.810 |
| Fib | -0.240 | 0.016 | 0.019 | 0.853 |
| TAT | 0.398 | 0.000 | -0.120 | 0.234 |
| tPAIC | 0.367 | 0.003 | 0.063 | 0.535 |
| PIC | 0.512 | 0.000 | 0.112 | 0.267 |
| sTM | 0.355 | 0.000 | 0.025 | 0.803 |
Diagnostic efficacy of coagulation markers and coagulation function indices for sepsis DIC
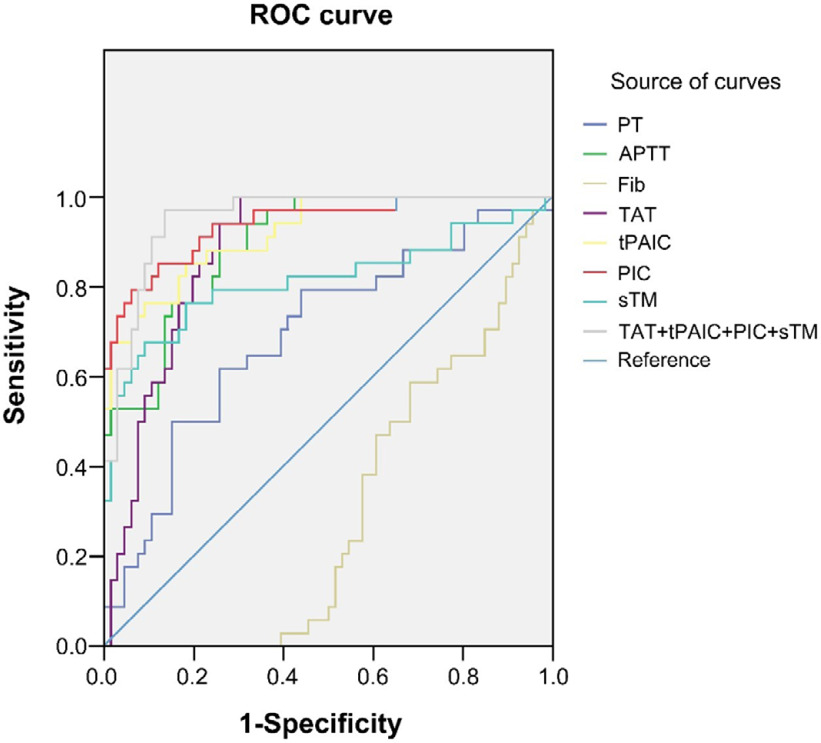
The results of the diagnostic efficacy of coagulation function and coagulation markers in the diagnosis of sepsis DIC are shown in Table 6 and Figure 1. The results indicated that while the diagnostic performance of Fib (AUC < 0.5) was suboptimal, all other indices demonstrated satisfactory diagnostic efficacy.
Table 6 Diagnostic efficacy of coagulation markers and coagulation function indices for sepsis DIC
| Sensitivity (%) | Specificity (%) | Jordon’s Index | AUC (95%CI) | |
|---|---|---|---|---|
| PT | 61.80 | 74.20 | 36.00 | 0.695 (0.584-0.806) |
| APTT | 88.20 | 74.20 | 62.40 | 0.896 (0.837-0.955) |
| Fib | 59.80 | 48.50 | 42.70 | 0.302 (0.201-0.402) |
| TAT | 82.40 | 69.70 | 66.80 | 0.883 (0.818-0.947) |
| tPAIC | 85.30 | 81.80 | 67.10 | 0.922 (0.869-0.975) |
| PIC | 79.40 | 93.90 | 73.30 | 0.939 (0.890-0.989) |
| sTM | 67.60 | 90.90 | 58.50 | 0.814 (0.710-0.917) |
| TAT+tPAIC+PIC+sTM | 97.10 | 86.40 | 83.50 | 0.954 (0.917-0.990) |
Figure 1 ROC curves of different indices in the diagnosis of sepsis-induced DIC.
The diagnostic effect of combining all four coagulation indicators (TAT+ tPAIC + PIC + sTM) exhibited the biggest area under the AUC curve, sensitivity of 97.10%, specificity of 86.40%, and a Youden index of 83.50%, indicating the highest diagnostic efficacy.
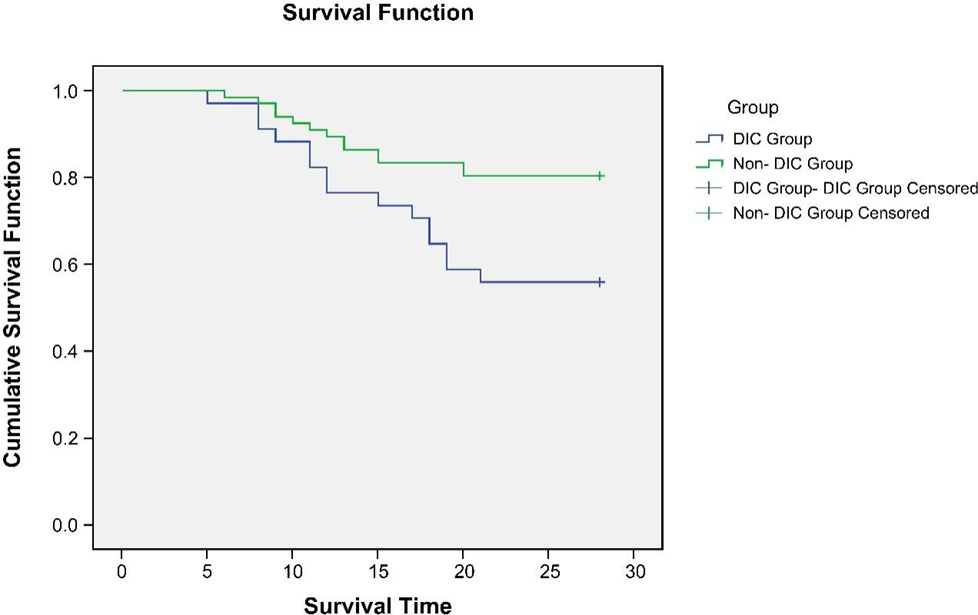
Comparison of 28-day survival of patients in two groups
According to statistics, 14 patients in the non-DIC group died in 28 days, with a mortality rate of 21.21%, while 15 patients in the DIC group died with a mortality rate of 44.12%. There was a significant difference in the mortality rate between the two groups (chi-square value = 5.718, p = 0.017). The mean survival value of the DIC group was 24.924 (23.362–26.486), and there was a significant difference between the two groups [Log Rank (Mantel-Cox) = 6.529, p=0.011]. The survival curve is shown in Figure 2.
Figure 2 Survival curves at 28 days for both groups.
Diagnostic efficacy of coagulation markers and coagulation function indices on prognosis
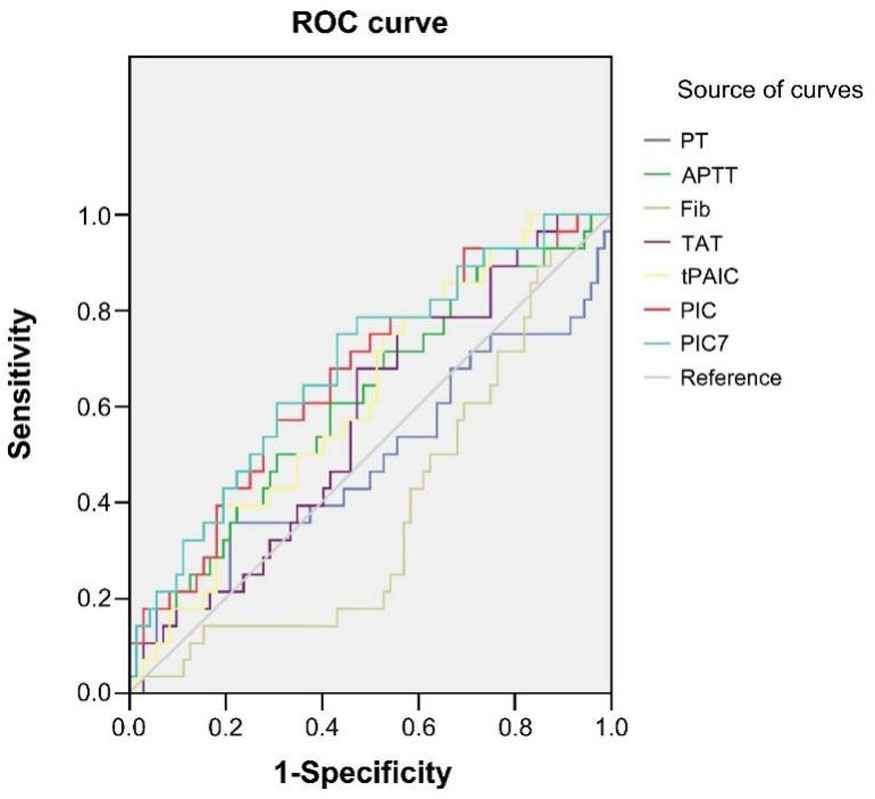
The predictive power of four coagulation markers and coagulation function indices regarding the prognosis of patients with sepsis is illustrated in Figure 3 and Table 7. The results of the ROC curve show that PT, Fib, and TAT are not effective in prognosis, as the area under the AUC curve of all three was less than 0.5. The AUC of APTT, tPAIC, PIC, and sTM was more than 0.5, which indicated that they have relevant diagnostic efficacy. The diagnostic effect of combining all four coagulation indicators (TAT+ tPAIC + PIC + sTM) was the best, with a sensitivity of 78.60%, a specificity of 70.80%, and a Youden index of 73.30%.
Table 7 Diagnostic efficacy of coagulation markers and coagulation function indices on prognosis.
| Sensitivity | Specificity | Jordon’s Index | AUC (95%CI) | |
|---|---|---|---|---|
| PT | 35.70 | 79.20 | 14.90 | 0.486 (0.348-0.624) |
| APTT | 50.00 | 69.40 | 19.40 | 0.610 (0.486-0.733) |
| Fib | 17.90 | 43.10 | 21.70 | 0.386 (0.268-0.505) |
| TAT | 71.00 | 69.70 | 66.80 | 0.572 (0.452-0.692) |
| tPAIC | 72.00 | 52.80 | 62.22 | 0.617 (0.500-0.734) |
| PIC | 57.10 | 69.40 | 56.50 | 0.661 (0.543-0.779) |
| sTM | 71.00 | 66.70 | 68.10 | 0.620 (0.487-0.753) |
| TAT+tPAIC+PIC+sTM | 78.60 | 70.80 | 73.30 | 0.681 (0.566-0.797) |
Figure 3 The diagnostic efficacy of four coagulation markers and coagulation function indices on the prognosis of patients with sepsis.
Discussion
Disseminated intravascular coagulation is not an independent disease but rather caused by a variety of diseases accompanied by coagulation dysfunction. The advancement of these underlying conditions may result in shock, multiple organ failure, and severe infections, particularly sepsis. Sepsis is a prevalent trigger of DIC, presenting a challenging health issue within acute and critical care settings, due to its substantial morbidity and mortality rates.17 There is no single definitive test for DIC in current clinical studies.18 Prior research has shown that clotting abnormalities in sepsis result from a complex interplay between inflammation and coagulation.19 In the study, both the DIC group and the non-DIC group exhibited mean atypical expression levels of inflammatory markers, suggesting that both groups experienced significant inflammatory pressure. While patients in the DIC group had elevated average levels of TNF-α, CRP, and IL-6 compared to those in the non-DIC group, the differences between the groups were not statistically significant. It is theorized that various inflammatory factors may exert distinct functions in sepsis and across the various phases of sepsis-induced DIC. However, the precise mechanisms require further investigation and understanding.
The determination of DIC in this study was mainly based on the ISTH criteria,20 as well as PT, APTT, and Fib, which are more readily available in the clinic and are commonly used coagulation indicators. In this study, we found that the APTT levels of patients in the DIC group were significantly higher than those in the non-DIC group on days 1, 3, and 7, whereas the Fib levels of this group were significantly lower than those of the non-DIC group during the same time period. The results of the study revealed that increased APTT and decreased Fib levels could potentially serve as early indicators for the onset of sepsis-induced DIC. SOFA score is an indicator that reflects the degree of organ damage and predicts the prognosis of patients, and is also one of the diagnostic indicators of sepsis.21 The APACHE II scoring system evaluates acute physiological derangement, pre-existing health conditions, and patient age. It is a commonly employed tool in clinical settings to gauge the severity of critical illness. Additionally, the system provides insights into the progression and prognosis of patients with severe medical conditions.22 The results of correlation analysis also confirmed that PT and APTT were positively correlated with SOFA score, while Fib was negatively correlated with SOFA score, which indicated that the three tests could not assess the severity of the patient's condition, but could only assist in the diagnosis of DIC occurrence. In addition, the ROC curve results showed that the AUC of PT and APTT were 0.695 and 0.896, indicating that they have a certain degree of diagnostic efficacy.
sTM, TAT, PIC, and t-PAIC are the four neo-coagulation items, and numerous studies in recent years have confirmed that these four neo-coagulation items have certain clinical guidance in the diagnosis of DIC.23 This phenomenon is evident not only in diagnosing DIC in individuals with blood cancer but also suggests that plasma sTM expression levels can serve as a crucial measure for assessing the status of patients with myeloma to some extent.24 During the early anticoagulation treatment of patients with acute exacerbation of chronic obstructive pulmonary disease (COPD), monitoring their index levels can guide the use of anticoagulants and potentially improve prognosis.25 Prevailing research has substantiated that these four parameters exhibit significant diagnostic value in the context of acute deep vein thrombosis.26 In this study, we found that the levels of sTM, TAT, PIC, and t-PAIC in the DIC group were significantly higher than those in the non-DIC group on days 1, 3, and 7. The outcomes of correlation analysis further validated that the levels of the four indices demonstrated a substantial positive correlation with the SOFA score. Conversely, there was no significant correlation observed with the APACHE II score, indicating that the four neo--coagulation parameters may not effectively assess the severity of the condition in sepsis-induced DIC patients.
The AUC curve areas of the four indexes ranged from 0.814 to 0.939, all of which were higher than 0.5. The diagnostic effect of combining all four coagulation indicators (TAT+ tPAIC + PIC + sTM) exhibited the largest area under the AUC curve (0.954), sensitivity of 97.10%, specificity of 86.40%, and a Youden index of 83.50%, indicating the highest diagnostic efficacy.
Finally, this study found that the mortality rate in the DIC group was significantly higher at 44.12% compared to 21.21% in the non-DIC group., This finding is consistent with the previously reported theories that patients with significant DIC tend to experience higher mortality rates.27 The survival curve analysis confirmed a significant disparity in survival rates between the two groups. Additionally, while the combination of TAT+ tPAIC + PIC + sTM demonstarted the best diagnostic value in this study, it was not the highest in terms of its sensitivity 78.60%, specificity 70.80%, and Jordon's index 73.30%. As a result, the findings show that the accuracy of coagulation indices and markers in diagnosing prognosis remains insufficient. Therefore, it is crucial to increase the research sample size and conduct a more in-depth investigation into this study.
This study has limitations, including a small sample size that was not estimated using a formal calculation method and a non-standardized selection process. To validate the results of this exploratory investigation into the early prediction of DIC in sepsis patients, a larger dataset is needed to strengthen the findings. In conclusion, detecting coagulation parameters and four coagulation markers is crucial for predicting the onset of sepsis-induced DIC, assessing disease severity, and determining prognosis. When combined, all four coagulation indicators exhibit strong diagnostic capability in identifying early-stage sepsis-induced DIC.
Acknowledgments
Not applicable.
Funding
This work was supported by Jiangxi Provincial Health Commission Science and Technology Project (Grant No. 202210579).
Conflicts of interest
The authors state that there are no conflicts of interest to disclose.
Ethics approval
Ethical approval was obtained from the Ethics Committee of The Second Affiliated Hospital, Jiangxi Medical College, Nanchang University.
Consent to participate statement
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Data availability
The authors declare that all data supporting the findings of this study are available within the paper and any raw data can be obtained from the corresponding author upon request.
Contribution of authors
Xiaowei Fang and Wei Fu designed the study and carried them out, Xiaowei Fang, Wei Fu, Luyang Xu, and Yichao Qiu supervised the data collection, analyzed the data, interpreted the data, Xiaowei Fang and Wei Fu prepared the manuscript for publication and reviewed the draft of the manuscript. All authors have read and approved the manuscript.
REFERENCES
1. Chiu C, Legrand M. Epidemiology of sepsis and septic shock. Curr Opin Anesthesio. 2021;34(2):71–6. 10.1097/ACO.0000000000000958
2. DeMerle KM, Angus DC, Baillie JK, Brant E, Calfee CS, Carcillo J, et al. Sepsis subclasses: A framework for development and interpretation. Crit Care Med. 2021;49(5):748–59. 10.1097/CCM.0000000000004842
3. Oczkowski S, Alshamsi F, Belley-Cote E, Centofanti JE, Moller MH, Nunnaly ME, et al. Surviving sepsis campaign guidelines 2021: Highlights for the practicing clinician. Pol Arch Intern Med. 2022;132(7–8):16290. 10.20452/pamw.16290
4. Kingren MS, Starr ME, Saito H. Divergent sepsis pathophysiology in older adults. Antioxid Redox Sign. 2021;35(16):1358–75. 10.1089/ars.2021.0056
5. Yang K, Chen JQ, Wang T, Zhang Y. Pathogenesis of sepsis--associated encephalopathy: More than blood-brain barrier dysfunction. Mol Biol Rep. 2022;49(10):10091–9. 10.1007/s11033-022-07592-x
6. Iba T, Levi M, Thachil J, Levy JH. Disseminated intravascular coagulation: The past, present, and future considerations. Semin Thromb Hemost. 2022;48(08):978–87. 10.1055/s-0042-1756300
7. Popescu NI, Lupu C, Lupu F. Disseminated intravascular coagulation and its immune mechanisms. Blood. 2022;139(13):1973–86. 10.1182/blood.2020007208
8. Schizas N, Nazou G, Antonopoulos C, Angouras DC. Disseminated intravascular coagulation post endovascular aortic repair. Vasc Endovasc Surg. 2023;57(7):738–48. 10.1177/15385744231165231
9. Matsumoto H, Annen S, Mukai N, Ohshita M, Murata S, Harima Y, et al. Circulating syndecan-1 levels are associated with chronological coagulofibrinolytic responses and the development of disseminated intravascular coagulation (DIC) after trauma: A retrospective observational study. J Clin Med. 2023;12(13):4386. 10.3390/jcm12134386
10. Zhang J, Xue MM, Chen Y, Liu CL, Kuang ZS, Mu SC, et al. Identification of soluble thrombomodulin and tissue plasminogen activator-inhibitor complex as biomarkers for prognosis and early evaluation of septic shock and sepsis--induced disseminated intravascular coagulation. Ann Palliat Med. 2021;10(10):10170–10184. 10.21037/apm-21-2222
11. Ikezoe T. Advances in the diagnosis and treatment of disseminated intravascular coagulation in haematological malignancies. Int J Hematol. 2021;113(1):34–44. 10.1007/s12185-020-02992-w
12. Yamada S, Asakura H. Therapeutic strategies for disseminated intravascular coagulation associated with aortic aneurysm. Int J Molec Sci. 2022;23(3):1296. 10.3390/ijms23031296
13. Jacobi J. The pathophysiology of sepsis-2021 update: Part 2, organ dysfunction and assessment. Am J Health-Syst Ph. 2022;79(6):424–36. 10.1093/ajhp/zxab393
14. Bateman RM, Sharpe MD, Jagger JE, Ellis CG, Solé-Violán J, López-Rodríguez M, et al. 36th International Symposium on Intensive Care and Emergency Medicine: Brussels, Belgium. 15–18 March 2016. Crit Care (London, England). 2016;20(Suppl 2):94.
15. Lee YT, Wang CC, Li CF, Chen HY, Liao HH, Lin CC. Utility of acute physiology and chronic health evaluation (APACHE II) in predicting mortality in patients with pyogenic liver abscess: A retrospective study. J Clin Med. 2021;10(12):2644. 10.3390/jcm10122644
16. Qiu X, Lei YP, Zhou RX. SIRS, SOFA, qSOFA, and NEWS in the diagnosis of sepsis and prediction of adverse outcomes: A systematic review and meta-analysis. Expert Rev Anti-Infe. 2023;21(8):891–900. 10.1080/14787210.2023.2237192
17. Adelborg K, Larsen JB, Hvas AM. Disseminated intravascular coagulation: Epidemiology, biomarkers, and management. Brit J Haematol. 2021;192(5):803–18. 10.1111/bjh.17172
18. Iba T, Helms J, Connors JM, Levy JH. The pathophysiology, diagnosis, and management of sepsis-associated disseminated intravascular coagulation. J Intensive Care. 2023;11(1):24. 10.1186/s40560-023-00672-5
19. Joffre J, Hellman J. Oxidative stress and endothelial dysfunction in sepsis and acute inflammation. Antioxid Redox Sign. 2021;35(15):1291–307. 10.1089/ars.2021.0027
20. Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11):E1063-E1143.
21. Liu H, Zhang LM, Xu FS, Li SJ, Wang ZC, Han DD, et al. Establishment of a prognostic model for patients with sepsis based on SOFA: A retrospective cohort study. J Int Med Res. 2021;49(9):3000605211044892. 10.1177/03000605211044892
22. Erdogan M, Findikli HA. Novel biomarker for predicting sepsis mortality: Vitamin D receptor. J Int Med Res. 2021;49(8):3000605211034733. 10.1177/03000605211034733
23. Unar A, Bertolino L, Patauner F, Gallo R, Durante-Mangoni E. Pathophysiology of disseminated intravascular coagulation in sepsis: A clinically focused overview. Cells-Basel. 2023;12(17):2120. 10.3390/cells12172120
24. Comerford C, Glaveyz S, O’Sullivan JM, Quinn J. Potential mechanisms of resistance to current antithrombotic strategies in Multiple Myeloma. Cancer Drug Resist. 2022;5(1):214–28. 10.20517/cdr.2021.115
25. Halpin DMG, Criner GJ, Papi A, Singh D, Anzueto A, Martinez FJ, et al. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. The 2020 GOLD Science Committee Report on COVID-19 and Chronic Obstructive Pulmonary Disease. Am J Resp Crit Care. 2021;203(1):24–36. 10.1164/rccm.202009-3533SO
26. Mazzolai L, Ageno W, Alatri A, Bauersachs R, Becattini C, Brodmann M, et al. Second consensus document on diagnosis and management of acute deep vein thrombosis: Updated document elaborated by the ESC Working Group on aorta and peripheral vascular diseases and the ESC Working Group on pulmonary circulation and right ventricular function. Eur J Prev Cardiol. 2022;29(8):1248–63. 10.1093/eurjpc/zwab088
27. Umemura Y, Nishida T, Yamakawa K, Ogura H, Oda J, Fujimi S. Anticoagulant therapies against sepsis-induced disseminated intravascular coagulation. Acute Med Surg. 2023;10(1):e884. 10.1002/ams2.884