
Download
CASE REPORT
Alpha-gal syndrome: when treatment of hypovolemic shock can lead to anaphylaxis
Francesca Nalina†, Rocco Scarmozzinob†, Alessandra Arcolacib, Bianca Olivieria, Marina Tommasic, Patrizia Bonadonnaa, Giovanna Zanonib*
aAllergy Unit, University Hospital, Azienda Ospedaliera Universitaria Integrata Verona, Italy
bImmunology Unit, University Hospital, Azienda Ospedaliera Universitaria Integrata Verona, Italy
cDepartment of Pharmacy, Azienda ULSS 9 Scaligera, Verona, Italy
†These authors contributed equally to this article
Abstract
Delayed anaphylaxis after ingestion of red meat because of galactose-alpha-1,3-galactose (alpha-gal) syndrome has increased in recent years. The mechanism involves an immunoglobulin E reaction to alpha-gal, a molecule found in mammalian meat, dairy products, medications and excipients containing mammalian-derived components, and tick salivary glycans. Sensitization occurs due to the bite of a lone star tick and the transmission of alpha-gal molecules into person's bloodstream. We describe a case of alpha-gal syndrome with severe food, drug, and perioperative allergy in which anaphylaxis with hypovolemic shock occurred immediately after an emergency surgical procedure, when a gelatin-containing drug was injected. This case study confirms that the clinical manifestations of alpha-gal syndrome could be different depending on the route of administration, with immediate reactions if an alpha-gal-containing drug is injected and delayed type allergic manifestations occurring several hours after oral intake. The purpose of this report is to highlight the importance of risk communication in case of exposure to medical products and surgical procedures of patients with alpha-gal syndrome and to encourage drug manufacturers to indicate clearly the origin of excipients in product literature.
Key words: alpha-gal syndrome, anaphylaxis, drug allergy, meat allergy
*Corresponding author: Giovanna Zanoni, Immunology Unit, University Hospital, Piazzale Scuro, 10, 37134 Verona, Italy. Email address: [email protected]
Received 15 January 2024; Accepted 1 March 2024; Available online 1 May 2024
Copyright: Nalin F, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
The term galactose-alpha-1,3-galactose (alpha-gal) syndrome describes an immunoglobulin E (IgE)-mediated allergy to disaccharide alpha-gal present on the surface of most non-primate mammalian cells and similar to blood group B antigen.1 It is synthesized by alpha-(1,3)-galactosyltransferase, which couples a terminal residue of galactose in an alpha-linkage to another galactose. Alpha-(1,3)-galactosyltransferase displays a peculiar pattern in mammals, as its expression is suppressed in primates, including humans, apes, and Old World monkeys;2 consequently, this disaccharide is immunogenic for humans.3
This syndrome was initially described in a group of patients with cancer who manifested immediate hypersensitivity reactions to the first infusion of monoclonal antibody cetuximab, in which alpha-gal is located on the fragment antigen-binding (Fab) region. Alpha-gal syndrome is one of the three dominant forms of IgE-mediated red meat allergy and differs from primary beef allergy and pork-cat syndrome regarding the onset of symptoms and route of sensitization.
The alpha-gal syndrome generally occurs in subjects previously sensitized to this oligosaccharide by tick bites and after consuming meat without problem for many years.4 An unknown factor in Amblyomma americanum (lone star tick) and other tick bites induces an IgE response to alpha-gal. Theories include a response to normal tick saliva constituents, residual mammalian glycoproteins or glycolipids containing alpha-gal present in the tick from a previous blood meal, or the presence of another as yet undescribed organism living in the tick.5 Ixodes ricinus, the castor bean tick, is the most widespread tick species in Europe and has been reported to contain alpha-gal in the midgut.6 In previous studies, patients with alpha-gal syndrome reported a higher proportion of allergic reactions following insect stings and were more likely to be sensitized to honey bee and wasp or fire ant than patients without this allergy.7 Increased levels of alpha-gal IgE were described following Hymenoptera sting.8 Moreover, a few patients were reported who did not express blood group B antigen anaphylactic transfusion reactions possibly because of IgE to alpha-gal.9
The main feature of this syndrome is the delayed onset of clinical manifestations (localized hives, angioedema, abdominal cramps, and anaphylaxis) 2–6 h after the ingestion of products of mammalian origin. The delay is explained by the time required for lipids to be packaged into chylomicrons by epithelial cells, and for these chylomicrons to transit to the systemic circulation via the thoracic duct, and for dietary lipids, including those bearing alpha-gal, to transition to other lipoprotein particles, such as low-density lipoproteins, which are small enough to exit from the vasculature into the interstitium, where mast cells reside.10 The risk and the severity of allergic reactions are related to the amount of alpha-gal present in food and drugs. The route of administration is relevant for the speed of onset of reactions: intravenous administration triggers rapid reactions whereas oral ingestion is associated with a delayed onset. Cofactors to allergic responses, such as the intake of non-steroidal anti-inflammatory drugs (NSAID), exercise, and alcohol could be additional risk modifiers.11 The diagnosis of red meat allergy often relies on a combination of clinical history, allergy skin tests, and determination of specific IgE. However, asymptomatic sensitization to meat allergens can be common in some populations.12 The sensitivity of skin prick testing is often inadequate for the diagnosis of red meat allergy.13 Measurement of specific IgE to alpha-gal and meat in serum has the advantage of being both highly sensitive and well-tolerated.14,15 Blood levels of IgE to alpha-gal often drop in patients who avoid recurrent tick bites, but the proportion of decline varies.16 The diagnosis also dictates the primary treatment, which is avoidance of mammalian meat (and also dairy products in some cases) and emergency plans, which include availability of epinephrine autoinjector. There are many ways in which food and other substances that are not obviously mammalian could nonetheless have mammalian products added during preparation or production. Evidence for the presence of alpha-gal in different foods and medicines varies widely, with some drugs clearly expressing the oligosaccharide (i.e., cetuximab) and other products considered potentially risky because they may contain some constituents of animal origin, such as magnesium stearate.17–19 Other products potentially dangerous for alpha-gal allergic subjects include heart valves, gelatin-based plasma expanders, pancreatic enzymes, and vaccines (Table 1).11 In the present paper we present the case of a severe drug, food, and perioperative allergy because of alpha-gal hypersensitivity.
Table 1: Products that may contain alpha-gal residues.
| Type of product | Source |
|---|---|
| Foods | Mammalian meat: beef, pork, lamb, deer, rabbit, horse, sheep, mutton, dolphin, and whale Dairy products: milk, cheese, yogurt, and butter Gelatin-containing sweets: marshmallows and jelly |
| Drugs | Cetuximab, infliximab Gelatin-based colloid plasma substitutes Pancreatic enzymes |
| Drug excipients | Gelatin (animal) Stearic acid Magnesium stearate Glycerin Lactic acid |
| Vaccines | Gelatin-containing vaccines (MMR, live attenuated varicella and zoster vaccines, yellow fever) |
| Other products | Bovine and porcine heart valves, collagen implants, sutures, contact lenses, shampoos, suppositories, and carrageenan (E407) |
MMR: measles, mumps, and rubella vaccine.
Case report
A 40-year-old man, cow breeder living in the mountains, was referred to our clinic with history of allergic rhinitis to house dust mites, cat and dog epithelium, and episodes of acute urticaria not related to specific substances. Allergy testing positivity to cow’s milk and beef was reported in the past, hence these foods were eliminated from his diet. The patient’s clinical history also established IgE-mediated sensitization to honey bee and wasp venom without evidence for systemic reactions to insect stings. The patient reported a recent episode of urticaria and angioedema 4 h after a meal with boiled beef meat and an episode of anaphylaxis with urticaria and hypotension 4 h after eating a ham and cheese sandwich and taking oral naproxen for headache. Alpha-gal syndrome was therefore suspected and confirmed by specific IgE determination, which was strongly positive to alpha-gal (>100 kU/L; normal values < 0.35 kU/L) and mammalian meat, while IgE to bovine gelatin was negative. The patient also reported symptoms of allergic rhinitis, conjunctivitis, and urticaria, while working in contact with cattle and positivity of specific IgE reactions to cow’s dander confirmed inhalant allergen sensitization. He was advised to exclude cow’s milk and red meat from his diet, and emergency therapy, such as epinephrine autoinjector, was prescribed; also, he was recommended to always carry rescue medications with him. Moreover, owing to suspected allergy to naproxen as an alternative NSAID, a challenge test with nimesulide in fractionated doses was performed in the hospital, showing tolerance to this drug.
In 2019, the patient was admitted to the emergency room for an episode of severe headache and was hospitalized in the Neurosurgery Unit for the evidence of cerebral bleeding confirmed by computed tomography (CT) of the brain. He underwent surgical clipping of two cerebral aneurysms. Immediately after surgery, he had anaphylactic shock with severe hypotension (blood pressure: 50/20 mmHg), tachycardia (heart rate 109 bpm), and bronchoconstriction (saturation 82% in intubated patient); he was treated with epinephrine, H1-antihistamine, and corticosteroids with prompt recovery. We reviewed the records of perioperative administered drugs and discovered that a plasma expander containing gelatin was injected (Geloplasma; Infuplus, Barcelona, Spain). The bovine origin of gelatin was subsequently confirmed by the drug manufacturer.
After recovery, the patient was discharged with a personalized therapy for hypertension with safe drugs, free from mammalian-derived components. In fact, several oral medications contain magnesium stearate. The prescribed drugs were verified from manufacturers by hospital pharmacist that tablet excipients, such as magnesium stearate, were of vegetal origin (cocoa).
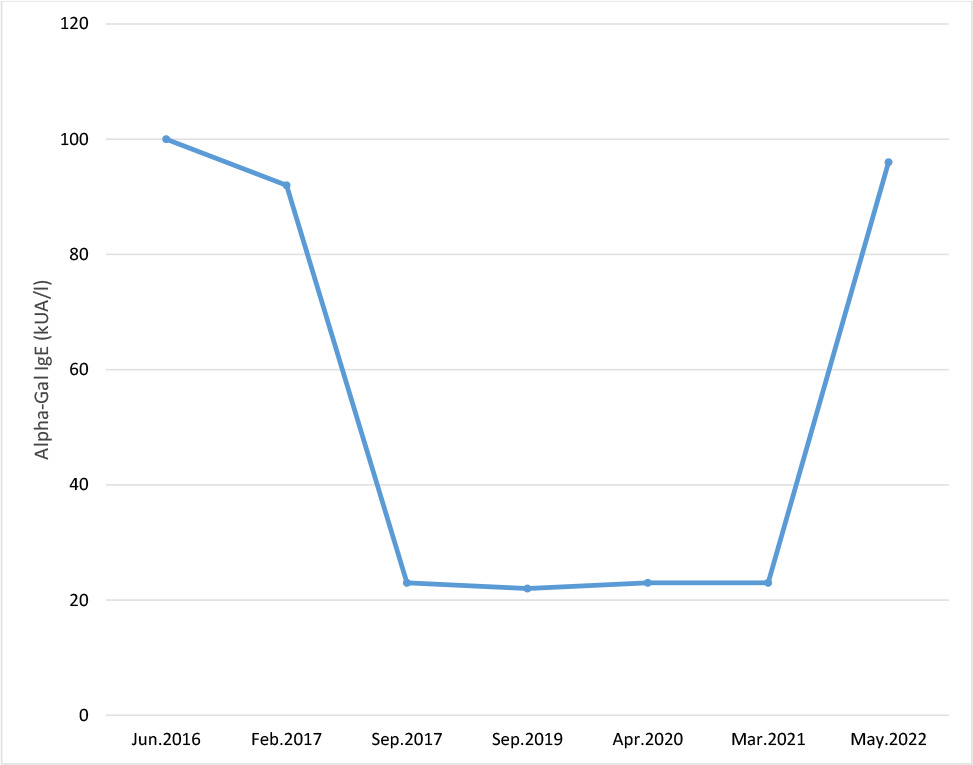
During follow-up, the patient did not report any further episodes of systemic allergic reactions, and specific IgE to alpha-gal decreased to 23 kU/L for a couple of years but subsequently climbed to 96 kU/L (Figure 1). He did not report further allergic reactions nor evident tick bites, although it appeared improbable due to the work-related exposition to parasites. Another possibility was that other arthropods or helminths could be responsible for the high level of IgE to alpha-gal, although further investigations are needed.20,21 During follow-up, although his IgE to alpha-gal remained high, he avoided consumption of mammalian meat and cow’s milk but tolerated other dairy products (i.e., cheese).
Figure 1: Levels of specific IgE to alpha 1-3 galactose (kU/L) from June 2016 to May 2022.
Discussion
Alpha-gal syndrome is a recently discovered clinical manifestation of drug and red meat allergy. Being a peculiar allergy, it is sometimes difficult to discern it because of delayed onset when the allergen is encountered by oral exposure.22 Besides common allergic manifestations, such as urticaria, angioedema, bronchospasm, and hypotension, nonclassical clinical manifestations involving only the gastrointestinal tract (GIT) with abdominal pain are described.11
Initial studies demonstrated that patients who reacted to cetuximab had a preexisting IgE to alpha-gal.23 Further observations of cases of adult-onset delayed anaphylaxis to red meat in the same rural areas of the United States, where the lone star tick (Amblyomma americanum) was endemic and reactions to cetuximab were described, suggested that bites from the lone star tick could be associated with sensitization to alpha-gal.24 The availability of in vitro tests to determine the presence of specific IgE to alpha-gal, together with detailed clinical history of reactions contributed to the identification of several additional cases outside the United States. A recent study conducted by Kersh et al. confirmed tick bite as a risk factor for alpha-gal syndrome and elevated alpha-gal-specific IgE.4
In our patient, work-related exposure to tick bites was the initial clue to suspect alpha-gal syndrome. A thorough medical history regarding his dietary regimen and potential cofactors of allergic reactions, such as NSAID, helped to determine a precise panel of allergy in vitro tests. Regarding respiratory manifestations, to our knowledge, this was the first case, and we did not determine any relationship between cow’s epithelium sensitization and alpha-gal syndrome.
Alpha-gal syndrome represents a multiple-drug allergy problem because of potential hypersensitivity to inactive substances, such as stearic acid, which are derived from either bovine or plant sources commonly present in oral medications.11,19 However, in the case of our patient, it was not possible to ascertain whether the manifestation after taking naproxen and ham was due to a cofactor mechanism or a reaction to magnesium stearate present in the drug.
Gelatin is administered as a plasma expander after surgical interventions, such as in our patient.11 The reaction could have been avoided in routine surgery; however, because of emergency hospitalization and intervention, our patient’s allergy history was not evaluated adequately. Allergy to red meat recorded in the patient’s history could be misleading regarding the possibility of triggering allergic reactions to drugs. Moreover, the patient’s condition contributed to underestimating this “food allergy,” while a thorough evaluation of the patient’s allergy history could have prevented an anaphylactic reaction to the plasma expander. As a precaution, patients with alpha-gal syndrome should be labeled as allergic to bovine and porcine gelatin to prevent any exposure to gelatin-containing products, even in cases of negative IgE to gelatin. Awareness of this syndrome must increase among surgeons and intensive care professionals to prevent serious allergic reactions.
Gelatin-containing vaccines, such as live attenuated zoster vaccine,25 and some brands of measles, mumps, and rubella (MMR) and varicella vaccines, include traces of animal gelatin and they can trigger immediate reactions in subjects sensitized to alpha-gal.19,26 In Italy, brands of these vaccines free from gelatin are available as alternative products and were recommended to our patient. No contraindications to other vaccines were recorded in the patient; in fact, he had a tetanus toxoid booster without adverse reactions.
Conclusion
In the last decade, alpha-gal syndrome has become a well-known entity worldwide, representing the most common type of delayed anaphylaxis. Drug reactions in alpha-gal syndrome have been documented and are quite variable in both severity and timing, probably because of the amount of alpha-gal present in the drug and the route of administration.
This case study is emblematic of showing different clinical manifestations of alpha-gal syndrome in relation to the route of administration to emphasize the importance of risk communication in case of exposure to medical products and for perioperative management of patients. Moreover, drug manufacturers are recommended to clearly indicate the origin of excipients in product literature. Further research is required to understand the degree of food and drug avoidance to be recommended to patients.11
Conflict of interest
The authors declared no conflict of interest.
Author contributions
Giovanna Zanoni and Francesca Nalin conceived and designed the paper; Francesca Nalin and Rocco Scarmozzino drafted the manuscript; Alessandra Arcolaci, Bianca Olivieri, Marina Tommasi, and Patrizia Bonadonna participated in the patient’s evaluation and critically revised the manuscript; Giovanna Zanoni provided the final approval of the version to be published.
REFERENCES
1. Fischer J, Yazdi AS, Biedermann T. Clinical spectrum of α-gal syndrome: From immediate-type to delayed immediate-type reactions to mammalian innards and meat. Allergo J Int. 2016;25(2):55–62. 10.1007/s40629-016-0099-z
2. Galili U, Shohet SB, Kobrin E, Stults CL, Macher BA. Man, apes, and Old World monkeys differ from other mammals in the expression of alpha-galactosyl epitopes on nucleated cells. J Biol Chem. 1988;263(33):17755–62.
3. Platts-Mills TAE, Schuyler AJ, Hoyt AEW, Commins SP. Delayed anaphylaxis involving IgE to galactose-alpha-1,3--galactose. Curr Allergy Asthma Rep. 2015;15(4):12. 10.1007/s11882-015-0512-6
4. Kersh GJ, Salzer J, Jones ES, Binder AM, Armstrong PA, Choudhary SK, et al. Tick bite as a risk factor for alpha-gal-specific immunoglobulin E antibodies and development of alpha-gal syndrome. Ann Allergy Asthma Immunol. 2023 Apr;130(4):472–8. 10.1016/j.anai.2022.11.021
5. Steinke JW, Platts-Mills TAE, Commins SP. The alpha-gal story: Lessons learned from connecting the dots. J Allergy Clin Immunol. 2015;135(3):589–96. 10.1016/j.jaci.2014.12.1947
6. Božan M, Vukičević Lazarević V, Marković I, Morović-Vergles J, Mitrović J. Alpha-gal syndrome–food or drug allergy: A case report. Clin Case Rep. 2023 Aug 24;11(9):e7830. 10.1002/ccr3.7830
7. Kutlu A, Unal D. Mammalian meat allergy accompanied by venom allergy: A review of 12 cases. Iran J Allergy Asthma Immunol. 2019 Oct 23;18(5):584–8. 10.18502/ijaai.v18i5.1928
8. Commins SP. Diagnosis & management of alpha-gal syndrome: Lessons from 2,500 patients. Expert Rev Clin Immunol. 2020 Jul;16(7):667–77. 10.1080/1744666X.2020.1782745
9. Gilstad CW, Conry-Cantilena K, Zarpak R, Eder AF. An outbreak of anaphylactic transfusion reactions to group B plasma and platelets and its possible relationship to alpha-gal syndrome. Transfusion. 2023 Oct;63(10):1997–2000. 10.1111/trf.17521
10. Wilson JM, Platts-Mills TAE. Red meat allergy in children and adults. Curr Opin Allergy Clin Immunol. 2019;19(3):229–35. 10.1097/ACI.0000000000000523
11. Platts-Mills TAE, Li R chi, Keshavarz B, Smith AR, Wilson JM. Diagnosis and management of patients with the α-gal syndrome. J Allergy Clin Immunol Pract. 2020;8(1):15–23.e1. 10.1016/j.jaip.2019.09.017
12. Fischer J, Lupberger E, Hebsaker J, Blumenstock G, Aichinger E, Yazdi AS, et al. Prevalence of type I sensitization to alpha-gal in forest service employees and hunters. Allergy. 2017;72(10):1540–7. 10.1111/all.13156
13. Orhan F, Sekerel BE. Beef allergy: A review of 12 cases. Allergy. 2003;58(2):127–31. 10.1034/j.1398-9995.2003.00021.x
14. Brestoff JR, Zaydman MA, Scott MG, Gronowski AM. Diagnosis of red meat allergy with antigen-specific IgE tests in serum. J Allergy Clin Immunol. 2017;140(2):608–10.e5. 10.1016/j.jaci.2017.01.032
15. Commins SP, Satinover SM, Hosen J, Mozena J, Borish L, Lewis BD, et al. Delayed anaphylaxis, angioedema, or urticaria after consumption of red meat in patients with IgE antibodies specific for galactose-alpha-1,3-galactose. J Allergy Clin Immunol. 2009;123(2):426–33. 10.1016/j.jaci.2008.10.052
16. Kim MS, Straesser MD, Keshavarz B, Workman L, McGowan EC, Platts-Mills TAE, et al. IgE to galactose-α-1,3-galactose wanes over time in patients who avoid tick bites. J Allergy Clin Immunol Pract. 2020 Jan;8(1):364–7.e2. 10.1016/j.jaip.2019.08.045
17. Ledward DA. Animal by-product processing by Ockerman H.W. & Hansen C.L.. Ellis Horwood Series in Food Science and Technology, VCH Verlagsgesellschaft, Weinheim, 1988. 366 pp. Price: (DM 250) £88. Meat Sci. 1989;26(2):163–4. 10.1016/0309-1740(89)90039-9
18. Muglia C, Kar I, Gong M, Hermes-DeSantis ER, Monteleone C. Anaphylaxis to medications containing meat byproducts in an alpha-gal sensitized individual. J Allergy Clin Immunol Pract. 3(5):796–7. 10.1016/j.jaip.2015.04.004
19. Dunkman WJ, Rycek W, Manning MW. What does a red meat allergy have to do with anesthesia? Perioperative management of alpha-gal syndrome. Anesth Analg. 2019 Nov 129(5):1242–8. 10.1213/ANE.0000000000003460
20. Stoltz LP, Cristiano LM, Dowling APG, Wilson JM, Platts-Mills TAE, Traister RS. Could chiggers be contributing to the prevalence of galactose-alpha-1,3-galactose sensitization and mammalian meat allergy? J Allergy Clin Immunol Pract. 2019 Feb;7(2):664–6. 10.1016/j.jaip.2018.07.014
21. Murangi T, Prakash P, Moreira BP, Basera W, Botha M, Cunningham S, et al. Ascaris lumbricoides and ticks associated with sensitization to galactose α1,3-galactose and elicitation of the alpha-gal syndrome. J Allergy Clin Immunol. 2022 Feb;149(2):698–707. 10.1016/j.jaci.2021.07.018
22. Commins SP, Jerath MR, Cox K, Erickson LD, Platts-Mills T. Delayed anaphylaxis to alpha-gal, an oligosaccharide in mammalian meat. Allergol Int. 2016 Jan;65(1):16–20. 10.1016/j.alit.2015.10.001
23. Chung CH, Mirakhur B, Chan E, Le QT, Berlin J, Morse M, et al. Cetuximab-induced anaphylaxis and IgE specific for galactose-alpha-1,3-galactose. N Engl J Med. 2008 Mar 13;358(11):1109–17. 10.1056/NEJMoa074943
24. Commins SP, James HR, Kelly LA, Pochan SL, Workman LJ, Perzanowski MS, et al. The relevance of tick bites to the production of IgE antibodies to the mammalian oligosaccharide galactose-α-1,3-galactose. J Allergy Clin Immunol. 2011 ,May;127(5):1286–93.e6. 10.1016/j.jaci.2011.02.019
25. Stone CA Jr, Hemler JA, Commins SP, Schuyler AJ, Phillips EJ, Peebles RS Jr, et al. Anaphylaxis after zoster vaccine: Implicating alpha-gal allergy as a possible mechanism. J Allergy Clin Immunol. 2017 May;139(5):1710–13. 10.1016/j.jaci.2016.10.037
26. Stone CA Jr, Commins SP, Choudhary S, Vethody C, Heavrin JL, Wingerter J, et al. Anaphylaxis after vaccination in a pediatric patient: Further implicating alpha-gal allergy. J Allergy Clin Immunol Pract. 2019 Jan;7(1):322–4. 10.1016/j.jaip.2018.06.005