
Download
ORIGINAL ARTICLE
Efficacy and perceived satisfaction of 3-year SLIT in children with allergic rhinitis and asthma: a pilot study
Sara Mantia,b*, Giulia Diletta Tropeab, Caterina Leddac, Giuseppe Fabio Parisib, Maria Papaleb, Enrico Compalatid, Franco Fratid, Salvatore Leonardib
aDepartment of Human Pathology in Adult and Developmental Age “Gaetano Barresi”, University of Messina, Messina, Italy
bDepartment of Clinical and Experimental Medicine, University of Catania, Catania, Italy
cOccupational Medicine, Department of Clinical and Experimental Medicine, University of Catania, Catania, Italy
dMedical Department, Lofarma S.p.A., Milan, Italy
Abstract
Background: Despite the presence of robust evidence, there is very limited data on the efficacy of allergen immunotherapy (AIT) for selected patients. Accordingly, we aimed to evaluate the efficacy and perceived satisfaction of a 3-year course of sublingual immunotherapy (SLIT) in a paediatric population with allergic rhinitis and/or asthma.
Methods: A pilot, monocentre, retrospective cohort study was performed. One hundred fifty-three children who fulfilled the criteria for allergic rhinitis and asthma and were either mono- or poly-sensitized were enrolled. A standardized questionnaire assessing perceived efficacy, use of rescue medication, disease control, number of exacerbations, quality of life, and perceived satisfaction was administered to each patient.
Results: Seventy patients (49 males, 21 females; mean age, 14.3±1.9 years) were included in the final analysis. All 70 patients received SLIT for up to 3 years, with 100% adherence to the treatment throughout the study. Significant improvements in symptoms and quality of life were reported (p<0.01). There was also a significant decrease in disease severity, use of rescue medication, and sleep disturbances (p<0.01). Additionally, a significant improvement in school performance was also recorded (p<0.01). Of the enrolled patients, 60 out of 70 (85.7%) reported being very satisfied, 6 out of 70 (8.57%) were much satisfied, and 4 out of 60 (5.71%) were satisfied.
Conclusions: We were the first to demonstrate the efficacy and perceived satisfaction of a 3-year SLIT in a paediatric population, with 100% treatment adherence throughout the study.
Key words: adherence, children, follow-up, perceived satisfaction, SLIT
*Corresponding author: Sara Manti, University Researcher, Pediatric Unit, Department of Human Pathology in Adult and Developmental Age “Gaetano Barresi”, University of Messina, Street Consolare Valeria, 1, 98124 Messina, Italy. Email address: [email protected]
Received 2 January 2024; Accepted 18 March 2024; Available online 1 November 2024
Copyright: Manti S, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
As confirmed by several randomized clinical trials (RCTs), consensus documents, and meta-analyses, allergen immunotherapy (AIT) has led to crucial improvements in clinical outcomes compared to standard treatments in selected patients. It is the only therapeutic approach capable of modifying the underlying course of the disease and achieving recovery from the disease.1–4
AIT aims to induce allergen-specific regulatory T (Treg) cells and promote the release of their anti-inflammatory cytokines, including interleukin (IL)-10, transforming growth factor (TGF-b), and surface molecules such as CTLA-4 and PD1. This modulation of T- and B-cell responses, mast cells, eosinophils and basophils results in the induction and maintenance of a long-term allergen-specific immune tolerance. Treg cells suppress Th2 cells, basophils, and eosinophils while also inducing allergen-specific Breg cells. Specifically, it is reported to block IgE production and an increase in IgG4 release from B cells.
Moreover, following the presentation of T-cell epitope peptides of allergens, naive T cells differentiate into T helper (Th) 2 cells that release Th2-type cytokines such as IL-4, IL-5, IL-9, and IL-13. These cytokines contribute to allergic inflammation: IL-4 and IL-13 activate B cells to class switch to IgE; and promote T cell and eosinophil migration to tissues. IL-5 promotes the recruitment and survival of eosinophils, IL-9 enhances IgE levels and eosinophilia, and IL-13 contributes to the production of mucus and smooth muscle contraction. AIT can block allergic inflammation by inhibiting all the mentioned mechanisms.
Therefore, AIT improves allergic symptoms and disease severity, decreases the need for rescue medication, and prevents new sensitizations.
Nevertheless, two major concerns remain regarding AIT in clinical practice: the benefits of adherence to AIT and its efficacy in real-life clinical practice.
To achieve disease modification, long-term immunological tolerance, significant improvement in symptoms, and reduction in rescue medication use, at least 3 years of AIT are recommended.1–4 However, even with adequate information on the advantages of AIT, it is comprehensible, especially in younger children, that patients and their parents may be hesitant to start the therapy due to its long duration. Therefore, it is crucial to clearly communicate to the patients and their caregivers the fruitful advantages they obtain by adopting this therapeutic strategy, even if for a long-time.
Despite the presence of robust evidence, there is very limited data5 available on the efficacy of AIT for selected patients in real-life settings. Real-life research methods, which consider the factors of daily clinical life, aim to evaluate the true effectiveness of innovative therapies.
Globally, RCTs are selected by the health sciences community as the main tool to investigate and evaluate clinical interventions with the lowest risk of bias. The adoption of inclusion and exclusion criteria, randomization, blinding, allocation, controlled environments, and other procedures help identify specific population groups who would benefit from the intervention and obtain statistically credible results.6 Nevertheless, the data obtained from RCTs may not always reflect the general population, making the translation and application of RCT findings to everyday clinical practice potentially questionable.
We strongly believe that real-world studies, using data collected in everyday clinical settings, can provide valuable insights to maximize the applicability and generalizability of an intervention.
Accordingly, we conducted a pilot, mono-centre, retrospective cohort study to evaluate real-life data on the efficacy and perceived satisfaction of a 3-year course of sublingual immunotherapy (SLIT), as measured by a validated questionnaire, in a population of mono- or poly-sensitized patients with allergic rhinitis and/or asthma. Moreover, to demonstrate that patients receiving AIT achieve significant clinical advantages, we chose to enrol patients with proven high therapeutic adherence. Accordingly, our study aims to provide real-life evidence that patients can gain fruitful advantages from adopting a long-term therapeutic strategy.
Materials and Methods
Study design
A pilot, monocentre, retrospective, open, real-life study was designed.
Objectives of the study
To evaluate, in real-life, the data on efficacy and perceived satisfaction of a 3-year course of SLIT in a population of mono- or poly-sensitized patients with allergic rhinitis and/or asthma.
Efficacy
The efficacy of the 3-year SLIT will be expressed as (1) perceived efficacy in patients; (2) rescue medication use; (3) disease control and impact on quality of life; and (4) number of disease exacerbations.
Satisfaction
The satisfaction of the 3-year SLIT will be expressed as (1) perceived satisfaction in patients; (2) quality of life in using patient-reported measures.
Subjects and eligibility criteria
One hundred fifty-three children who fulfilled the criteria for allergic rhinitis and asthma,5,6 and were referred to the Department of Clinical and Experimental Medicine, University of Catania between January 2016 and May 2022 were enrolled in the study.
Inclusion criteria were as follows: (i) patients of both sexes; (ii) ages 6-18 years old; (iii) diagnosed with allergic rhinitis, allergic asthma, or both, according to ARIA7 and GINA’s8 criteria, respectively; (iv) mono- or poly-sensitized to ambrosiae, artemisiae, betulaceae, dermatophagoides farinae and pteronyssinus, cat epithelium, grasses, olive and parietaria, as assessed by skin prick test (SPT); (v) treated preseasonally, coseasonally or continuously with grass pollen (ambrosiae, artemisiae, betulaceae, dermatophagoides farinae, and pteronyssinus, cat epithelium, grasses, olive and parietaria) tablets up to 3 years; (vi) stopped SLIT at least 3 years.
Exclusion criteria included: (i) children younger than 6 years or older than 18 years; (ii) patients diagnosed with chronic disease; (iii) patients who had stopped SLIT for less than 3 years.
Immunotherapy
SLIT was performed using a preparation of carbamylated allergoid (Lais®, Lofarma SpA, Milan, Italy), biologically standardised in allergenic units (AU, 1:1000 AU), prepared as orosoluble tablets (allergoid SLIT), and administered according to the manufacturer’s recommendations. Patients started with a maintenance dose of 1000 AU, taken regularly twice a week for house-dust mites and five times a week for pollens.
Study procedures
After identifying the patients who met the inclusion criteria, a physician administered a structured questionnaire regarding their experience with the past 3-year SLIT. The interview could be conducted in person or by telephone.
The questionnaire included an explanatory cover letter detailing the aim of the study. The questions were designed by the experts in the field.
The structured questionnaire was available as an online form with open-ended questions on the website. Responses were anonymous, but general information (initials of name and surname, age, gender, allergen for which SLIT was administered, drug administration schedule) was requested.
In accordance with the diagnosis (allergic rhinitis, allergic asthma, allergic rhinitis and asthma), three different questionnaires were administered. Patients who had undergone multiple cycles of SLIT were evaluated for each treatment using a specific questionnaire for each allergen.
Each questionnaire included 20 multiple-choice questions, and each questionnaire was divided into four time points: (i) T0: period prior to the start of therapy with monomeric carbamyl allergy; (ii) T1: first year of therapy with monomeric carbamyl allergy; (iii) T2: conclusion of the treatment with monomeric carbamyl allergoid; and (iv) T3: period following the suspension of treatment with monomeric carbamyl allergoid. Specifically, in accordance with European Academy of Allergy and Clinical Immunology (EAACI) recommendation,9 each questionnaire included questions on combined symptom and medication score, including:
-
Perceived efficacy: Measured using a visual analog scale (VAS) that has been proven to be a valid tool for evaluating patient satisfaction with allergic rhinitis.10 Using the VAS, patients assessed their level of satisfaction by indicating a position on a continuous line between two points from 0 (absence of symptoms) to 10 (bothersome or severe symptoms). The VAS was used for assessment at T0, T1, T2, and T3.
-
Rescue medication use: Measured using a VAS.10 Patients assessed the level of rescue medication use (antihistamines, inhaled or systemic corticosteroids) by indicating a position on a continuous line between two points from 0 (never used) to 10 (widely used). The VAS was used for assessment at T0, T1, T2, and T3.
-
Perceived efficacy: Measured using a visual analog scale (VAS) that has been proven to be a valid tool in evaluating patient satisfaction with asthma.8,11,12 Using the VAS, patients assessed their level for satisfaction by indicating a position on a continuous line between two points from 0 (absence of symptoms) to 10 (bothersome or severe symptoms). The VAS was used for assessment at T0, T1, T2, and T3.
-
Allergic rhinitis control and its impact on quality of life: Assessed through a standardized questionnaire according to ARIA guidelines.7 The questionnaire was used for assessment at T0 and T3.
-
Asthma control and its impact on quality of life: Assessed through standardized questionnaire according to GINA guidelines.8 The questionnaire was used for assessment at T0, T1, T2, and T3.
-
Number of asthma exacerbations: requiring the use of rescue therapy (salbutamol or systemic corticosteroids) or hospitalization in the last 12 months. This was measured on a scale from 0 to 8.
-
Perceived satisfaction: Expressed in terms of “very dissatisfied”, “dissatisfied”, “satisfied”, and “very satisfied”. Perceived satisfaction was assessed at T0, T1, T2, and T3.
One answer was provided for each question. The questionnaire was administered in Italian and translated into English for publication. The English version of the questionnaire is provided in Table 1A,B.
Table 1 English version of the questionnaire administered to patients with allergic rhinitis (A), asthma (B), rhinitis and asthma (A and B).
| (A) Allergic rhinitis | ||||
|---|---|---|---|---|
| T0 | T1 | T2 | T3 | |
| What is the level of severity and discomfort of nasal and ocular symptoms? | 0–10 | 0–10 | 0–10 | 0–10 |
| Rescue medication use (antihistamines, local and or systemic steroids) | 0–10 | 0–10 | 0–10 | 0–10 |
| How often your symptoms recurred? | •≤4 days/week •≤4 weeks |
•≤4 days/week •≤4 weeks | ||
| How long do your symptoms persist? | •≥ 4 days/ week •≥ 4 weeks |
•≥ 4 days/ week •≥ 4 weeks | ||
| Is sleep disturbed due to allergy? | •Yes •No |
•Yes •No | ||
| Have you had any limitations in daily work or school activities with reduced performance? | •Yes •No |
•Yes •No | ||
| Are your symptoms bothersome? | •Yes •No |
•Yes •No | ||
| Are your symptoms severe? | •Yes •No |
•Yes •No | ||
| How many years did you stop treatment? | •1 year •> 2 years | |||
| Are you satisfied with the treatment? | •Very dissatisfied •Dissatisfied •Satisfied •Very satisfied | |||
| (B) Asthma | ||||
| T0 | T1 | T2 | T3 | |
| What is the level of severity and discomfort symptoms? | 0–10 | 0–10 | 0–10 | 0–10 |
| Are daytime symptoms present more than 2/week? | •Yes •No |
•Yes •No |
•Yes •No |
•Yes •No |
| Are nighttime awakenings present due to symptoms? | •Yes •No |
•Yes •No |
•Yes •No |
•Yes •No |
| Did you use bronchodilators (salbutamol) several times a week? | •Yes •No |
•Yes •No |
•Yes •No |
•Yes •No |
| How many times did you use systemic steroids for asthmatic exacerbations? | 0–8 | 0–8 | 0–8 | 0–8 |
| How many years did you stop treatment? | •1 year •> 2 years | |||
| Are you satisfied with the treatment? | •Very dissatisfied •Dissatisfied •Satisfied •Very satisfied | |||
Safety was defined by the number and the type (mild, moderate, and severe) of adverse events (AEs) recorded by physician and/or children’s parents and/or patients.
Collected data were securely stored and managed using electronic data capture tools (server: PHP; Web: HTML, CSS, JS; Framework: Bootstrap; Libraries JS: jquery, noUiSlider).
Written informed consent was obtained in the study. For minors, consent was obtained from next of kin, caregivers, or guardians.13 Patient privacy was protected in compliance with the European Union General Data Protection Regulation (GDPR). The study was approved by the Institutional Review Board of University of Catania.
Data analysis
The data collected were statistically analysed using SPSS software, version 15.0. A post hoc analysis of temporal trends was performed. Descriptive statistics were calculated for all demographic and clinical variables. Continuous variables were presented as means and standard deviations(SD), while categorical variables were presented as frequencies and percentages. The normality assumption was verified using the Shapiro-Wilk test. For comparisons between categorical variables, T-student and χ2 tests were adopted, and for comparisons between continuous variables, both the T-test and non-parametric Mann-Whitney tests were employed. Kaplan-Meier curves were used to estimate survival functions. Statistical significance was set at levels of P < 0.05.
Results
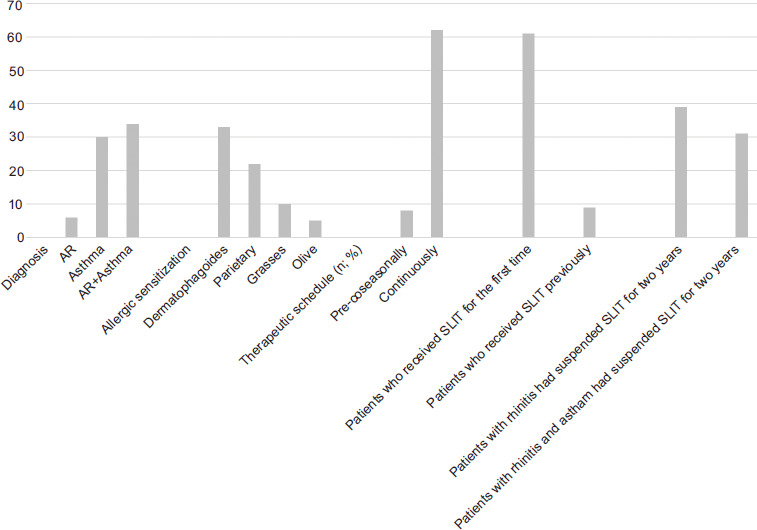
Out of 153 patients, 70 children were evaluated (49 males, 21 females; mean (SD) age, 14.3 ± 1.9 years; age range, 10-18). Eighty-three patients were lost at the follow-up since they retrieved the informed consents (num=33), changed residency (num= 14), changed phone number (num=17), and did not provide answers to all questions (num=19). The demographic and clinical characteristics, as well as sensitization details of the evaluated patients are reported in Table 2. All 70 patients received SLIT for up to 3 years, with 100% treatment adherence throughout the study. Among these 70 patients, 62 (89%) received SLIT continuously, while 8 (11%) received SLIT pre-coseasonally. No AEs were reported during the study.
Table 2 Demographic data and clinical characteristics of the enrolled patients.
| Patients, No | 70 |
|---|---|
| Age (Mean± SD) | 14.3 ± 1.9 |
| Gender No. M:F % M:F |
49:21 70%: 30% |
| Diagnosis (n; %) Allergic rhinitis Allergic asthma Allergic rhinitis and asthma |
6; 8.6% 30; 42.9% 34; 48.6% |
| Allergic sensitization (n; %) Dermatophagoides Parietary Grasses Olive |
33; 47.1% 22; 31.4% 10; 14.3% 5; 7.1% |
| Therapeutic schedule (n; %) Pre-coseasonally Continuously |
8; 11% 62; 89% |
| Patients who received SLIT for the first time (n; %) Patients who have received SLIT previously (n; %) |
61; 87% 9; 13% |
| Patients with rhinitis had suspended SLIT for two years (n; %) Patients with rhinitis and asthma had suspended SLIT for two years (n; %) |
39; 56% 31; 44% |
SD: standard deviation; M: male; F: female; SLIT: sublingualimmunotherapy.
Patients with allergic rhinitis with or without asthma
Of the 70 patients, 6 reported having allergic rhinitis. Among these 6 patients, 4 (75%) had moderate-to-severe intermittent allergic rhinitis, and 2 (25%) had moderate-to-severe persistent allergic rhinitis. Additionally, 34 out of 70 patients experienced allergic rhinitis with asthma. Except for 2 patients, 32 of the 34 (94.11%) reported moderate-to-severe intermittent allergic rhinitis.
At T3, a significant clinical improvement in nasal and eye symptoms was reported: T0: 7.7 ± 1.5 vs. T3: 2.4 ± 2.7 (p<0.01). There was also a significant decrease in disease severity (T0: 8/40 (20%) vs. T3: 0/40 (100%), p<0.01), rescue medication use (T0: 6.4 ± 2.7 vs. T3: 2.4 ± 3.2 (p<0.01)), and sleep disturbances (T0: 19/40 (47.5%) vs. T3: 9/40 (22%), p<0.01).
Additionally, a significant improvement in school performance was also recorded: T0: 9/40 (22%) vs. T3: 2/40 (5%), p<0.01.
No significant changes were reported in frequency of symptoms (≤ 4 days/week or ≤ 4 weeks: T0: 26 (65%) or 14 (35%) vs. T3: 21 (52.5%) or 19 (47.5%); ≥ 4 days/week o ≥ 4 weeks: T0: 20 (50%) or 20 (50%) vs. T3: 28 (70%) or 12 (30%).
Patients with allergic asthma or allergic asthma and rhinitis
Of the 70 patients, 64 reported having asthma or allergic asthma with rhinitis. At T3, a significant clinical improvement was reported: T0: 7.6 ± 2.1 vs. T3: 0.9 ± 1.8 (p<0.01). In parallel, there was a significant decrease in frequency of symptoms (> 2 days/week: T0: 42/64 (66%) vs. T3: 1/64 (2%), p<0.01); rescue medication use (salbutamol: T0: 36/64 (56%) vs. T3: 1/64 (2%) (p<0.01); systemic corticosteroids: T0: 36/64 (56%) vs. T3: 1/64 (2%) (p<0.01)); and sleep disturbances (T0: 39/64 (61%) vs. T3: 64/64 (100%), p<0.01). A significant improvement in school performance was recorded: T0: 15/64 (23%) vs. T3: 2/64 (3%), p<0.01.
Perceived satisfaction for all enrolled patients
Of the 70 enrolled patients, 60 (85.7%) reported being very satisfied, 6 (8.57%) were much satisfied, and 4 (5.71%) were satisfied.
All results are summarized in Figure 1.
Figure 1 Characteristics of the enrolled population.
Discussion
We performed a pilot, monocentre, retrospective cohort study to evaluate the efficacy and perceived satisfaction of 3-year SLIT in a real-life setting. This was measured using a validated questionnaire, in a population of mono- or poly-sensitized patients with allergic rhinitis and/or asthma. As expected, SLIT significantly contributed in modifying the disease course in patients with allergic rhinitis, asthma as well asthma with rhinitis. The positive impact of the treatment has been assessed by significant changes in perceived efficacy in patients, rescue medication use; perceived satisfaction in patients; disease control and impact on quality of life; and number of disease exacerbations. Significant changes have also been recorded in the frequency of symptoms for patients with asthma and asthma with allergic rhinitis. However, no significant changes were reported in the allergic rhinitis group. The absence of significant changes related to the small sample size, with only six patients suffering from allergic rhinitis.
Confirming the efficacy of SLIT, the perceived satisfaction among all enrolled patients was high. It is reasonable to hypothesize that these data were related to the improvement in clinical outcome. Few studies have investigated the efficacy/perceived satisfaction ratio, which is crucial in obtaining a high treatment adherence.14–16 Moreover, when this issue was investigated, several biases were affecting the results, such as conflict of interests.14,15 In our study, all patients reported a high rate of satisfaction, likely due to the efficacy of the treatment. It has been reported that the reasons for the premature cessation of AIT are the inability to reach the clinical centre, the ineffectiveness of the therapy, and the long course of treatment.17 In this study, we were able to enrol patients who were highly motivated to start treatment and participate in the study without a strict protocol. All these factors resulted in high treatment adherence with 60 out of 70 (85.7%) patients declaring themselves very satisfied, 6 out of 70 (8.57%) much satisfied, and 4 out of 60 (5.71%) satisfied. Adherence is the key to ensuring the effectiveness of SLIT, as poor adherence can negatively affect the efficacy of AIT. In line with this finding, all enrolled patients completed at least 3 years of treatment, showing 100% spontaneous adherence to the prescribed treatment. In contrast to other studies where high treatment adherence was obtained through nurse interventions, frequent scheduled visits, and telephone calls,18–20 our patients showed 100% spontaneous adherence to the prescribed treatment. In this regard, we believe that the patients were obtaining genuine benefits from the treatment, probably from the first year of the therapy. Thus, good efficacy achieved during the first year of treatment could be considered a favourable prognostic factor for treatment adherence over the next 2 years, leading to long-lasting positive effects in real-world practice. Furthermore, only continuous AIT for a period of at least 3 years modifies the course of the disease and ensures long-term remission of symptoms for several years.21–24 RCTs and observational studies on treatment adherence have reported discontinuation rate for SCIT to be approximately 22%, 34%, and 26% from 1 to 3 treatment years, respectively, and, for SLIT of 42%, 29%, and 27% over the same period.25,26 In this study, we reported for the first time that the treatment adherence for SLIT was 100% throughout the study duration. Similar to other chronic conditions, allergic diseases require ongoing care to minimize their impact, improve health outcomes, prevent clinical worsening and comorbidities, and reduce healthcare costs.27 Nevertheless, it is estimated that only about half of patients with chronic conditions take their medications as prescribed, as several factors affect the patients’ ability to follow treatment recommendations correctly.27,28 We strongly believe that the complete treatment adherence observed in our population can be primarily attributed to the study design. In RCTs, patients are strictly selected and monitored over time to limit bias; those who differ from that set out are excluded from the final study results. Conversely, more reliable data can be derived from real-life studies, since a combination of strategies, such as educational plans and regular assessments, can be more easily implemented.29
Moreover, the novelty and strength of our study were lie in demonstrating the efficacy and perceived satisfaction of 3-year SLIT through a real-life design. Although the health sciences community often selects RCTs as the main tool to investigate and evaluate clinical interventions with the lowest risk of bias, the obtained data does not ever fit with the general population. Thus, the translation and the use of data obtained from RCTs in real-practice can be questionable. Specifically, in the context of AIT, several issues with RCTs contribute to their inadequacy. These studies generally have short durations and are limited to one pollen season. It is well known that the potential of AIT in preventing new sensitization and onset of allergic diseases is strictly correlated with the duration of the treatment, with a recommended minimum course of 3 years.30,31
RCTs are designed to test if the selected treatment is effective, but they do not evaluate if the treatment works in real-life. Aiming to limit any factor that could potentially influence results, RCTs are designed in compliance with a rigid and strict protocol. However, the protocols are not uniformly applied across all RCTs, leading to extensive “within-study” and “between-study” heterogeneity among different trials.6 Moreover, RCTs often investigate experimental treatments in a selected group of patients who meet the study’s inclusion criteria.6 Any protocol modification is foreseen for patients who do not strictly meet the inclusion criteria or for unforeseen events.6 Thus, certain patient groups (e.g., age, disease severity, comorbidities, use of concomitant medications, etc), from which it could be possible to extract potential and interesting data, may be excluded from the study. The exclusion criteria creates a gap in understanding how the treatment performs in real-practice.
On one hand the “one-size-fits-all” approach can provide a treatment applicable for a large population, while on the other hand, it does not work for everyone. A treatment defined as “effective” in an ideal clinical setting may not give specific quantifiable answers in individual cases within a routine clinical setting. A tailored healthcare approach and treatment to meet the specific needs of each patient. is urgently needed as only a “sartorial” approach can provide an individual’s unique molecular, lifestyle, and clinical information.
We strongly believe that real-world studies, which use data collected in everyday clinical settings, hold the promise of providing real data to maximize the applicability and generalizability of an intervention. Nevertheless, our aim is not to create a conflict between a “wrong” and “right” research approach, instead we aim to shift form a dichotomous to an integrated perspective that combines the strengths of each research method. This indicates the prospective, randomized, and analytical design of RCTs with the more representative and generalizable data from real-life studies. By doing so, we exceed the limits of restrictive inclusion and exclusion criteria of RCTs and the risk of low-quality control of the surrounding data collection and susceptibility to multiple sources of bias occurring in real-life studies.
Limits of the study
Nevertheless, we are aware that our study has limitations, as we designed a retrospective trial and included small numbers of patients. We are considering the possibility of designing a prospective study and also plan to conduct a larger study to increase the sample size. However, the small sample size is due to our decision to include only patients with 100% adherence to therapy and high motivation for treatment success. Therefore, our results did not reveal if AIT works even in case of low therapeutic adherence. However, it is widely reported that AIT is effective when it is taken adequately by the patient, and our study demonstrates that AIT works well under these conditions. This evidence represents a crucial motivation for patients approaching the AIT because they take responsibility for their well-being. When the treatment is taken adequately and constantly, patients can achieve several advantages, such as improved clinical symptoms, quality of life, and sparing symptomatic therapy.
Author Contributions
Conceptualization, FF and SL; methodology, CL; software, EC; FF; validation, SM, GD T; formal analysis, CL; investigation, GFP; MP; resources, FF; data curation, SM, GDT, CL; writing—original draft preparation, SM; writing—review and editing, SM, EC, FF; visualization, SL; supervision, FF, SL; project administration, FF.
Conflicts of Interest
EC and FF work in Lofarma. The remaining authors declare no conflict of interest.
REFERENCES
1 Frati F, Incorvaia C, Passalacqua G. Efficacy of sublingual immunotherapy. JAMA. 2013; 310(6):643–4. 10.1001/jama.2013.7646
2 Calamita Z, Saconato H, Bronhara Pelà A, Nagib Atallah A. Efficacy of sublingual immunotherapy in asthma. Systematic review of randomized clinical trials. Allergy. 2006; 61:1162–72. 10.1111/j.1398-9995.2006.01205.x
3 Melaranci C, Matteoli MC. Efficacy of allergoid sublingual immunotherapy in children with asthma and/or allergic rhinoconjunctivitis. JACI. 2004; 113:S111. 10.1016/j.jaci.2003.12.388
4 Cuppari C, Leonardi S, Manti S, Filippelli M, Alterio T, Spicuzza L, et al. Allergen immunotherapy, routes of administration and cytokine networks: an update. Immunotherapy. 2014; 6(6):775–86. 10.2217/imt.14.47
5 Pastorello EA, Losappio L, Milani S, Manzotti G, Fanelli V, Pravettoni V, et al. 5-grass pollen tablets achieve disease control in patients with seasonal allergic rhinitis unresponsive to drugs: a real-life study. J Asthma Allergy. 2013; 6:127–33. 10.2147/JAA.S53801
6 Kabisch M, Ruckes C, Seibert-Grafe M, Blettner M. Randomized controlled trials: part 17 of a series on evaluation of scientific publications. Dtsch Arztebl Int. 2011; 108(39):663–8. 10.3238/arztebl.2011.0663
7 Bousquet J, Khaltaev N, Cruz AA, et al. World Health Organization; GA(2)LEN; AllerGen. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 Update (in collaboration with the World Health Organization, GA2LEN and AllerGen). Allergy. 2008;63(Suppl. 86):8–160. 10.1111/j.1398-9995.2007.01620.x
8 Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. Available at: https://ginasthma.org/wp-content/uploads/2021/05/GINA-Main-Report-2021-V2-WMS.pdf. Last Access: July 26, 2022
9 Pfaar O, Demoly P, Gerth van Wijk R, Bonini S, Bousquet J, Canonica GW, et al. Recommendations for the standardization of clinical outcomes used in allergen immunotherapy trials for allergic rhinoconjunctivitis: an EAACI Position Paper. Allergy. 2014; 69(7), 854–867. 10.1111/all.12383
10 Klimek L, Bergmann KC, Biedermann T, Bousquet J, Hellings P, Jung K, et al. Visual analogue scales (VAS): Measuring instruments for the documentation of symptoms and therapy monitoring in cases of allergic rhinitis in everyday health care: Position Paper of the German Society of Allergology (AeDA) and the German Society of Allergy and Clinical Immunology (DGAKI), ENT Section, in collaboration with the working group on Clinical Immunology, Allergology and Environmental Medicine of the German Society of Otorhinolaryngology, Head and Neck Surgery (DGHNOKHC). Allergo J Int. 2017; 26(1):16–24. 10.1007/s40629-016-0006-7
11 Rhee H, Belyea M, Mammen J. Visual analogue scale (VAS) as a monitoring tool for daily changes in asthma symptoms in adolescents: a prospective study. Allergy Asthma Clin Immunol. 2017; 13:24. 10.1186/s13223-017-0196-7
12 Meltzer EO, Busse WW, Wenzel SE, Belozeroff V, Weng HH, Feng J, et al. Use of the asthma control Questionnaire to predict future risk of asthma exacerbation. J Allergy Clin Immunol. 2011; 127:167–172. 10.1016/j.jaci.2010.08.042
13 Manti S, Licari A. How to obtain informed consent for research. Breathe. 2018; 14(2):145–52. 10.1183/20734735.001918
14 De Vos C, Mitchev K, Pinelli ME, Derde MP, Boev R. Non-interventional study comparing treatment satisfaction in patients treated with antihistamines. Clin Drug Investig. 2008; 28:221–30. 10.2165/00044011-200828040-00003
15 Ferrer M, Morais-Almeida M, Guizova M, Khanferyan R. Evaluation of treatment satisfaction in children with allergic disease treated with an antihistamine: an international, non-interventional, retrospective study. Clin Drug Investig. 2010; 30:15–34. 10.2165/11530910-000000000-00000
16 Zicari AM, Indinnimeo L, De Castro G, Incorvaia C, Frati F, Dell’Albani I, et al. A survey on features of allergic rhinitis in children. Curr Med Res Opin. 2013; 29(5):415–20. 10.1185/03007995.2013.779238
17 Wang T, Li Y, Wang F, Zhou C. Nonadherence to sublingual immunotherapy in allergic rhinitis: a real-life analysis. Int. Forum Allergy Rhinol. 2017; 7:389–392. 10.1002/alr.21909
18 Kiotseridis H, Arvidsson P, Backer V, Braendholt V, Tunsäter A. Adherence and quality of life in adults and children during 3-years of SLIT treatment with Grazaxa real life study. NPJ Prim Care Respir Med. 2018; 28(1):4. 10.1038/s41533-018-0072-z
19 Ras L, de Groot H, Stengs CH, van Weissenbruch R. Persistence of treatment with 5-grass pollen tablets in patients with allergic rhinitis: a real-life study. Ann Allergy Asthma Immunol. 2016; 116(1):52–8.e2. 10.1016/j.anai.2015.10.018
20 Pajno GB, Caminiti L, Crisafulli G, Barberi S, Landi M, Aversa T, et al. Adherence to sublingual immunotherapy in preschool children. Pediatr Allergy Immunol. 2012; 23(7):688–9. 10.1111/j.1399-3038.2012.01317.x
21 Halken S, Larenas-Linnemann D, Roberts G, Calderón MA, Angier E, Pfaar O, et al. EAACI guidelines on allergen immunotherapy: prevention of allergy. Pediatr Allergy Immunol. 2017; 28(8):728–745. 10.1111/pai.12807
22 Valovirta E, Petersen TH, Piotrowska T, Laursen MK, Andersen JS, Sørensen HF, et al. Results from the 5-year SQ grass sublingual immunotherapy tablet asthma prevention (GAP) trial in children with grass pollen allergy. J Allergy Clin Immunol. 2018; 141(2):529–538 e513. 10.1016/j.jaci.2017.06.014
23 Eng PA, Borer-Reinhold M, Heijnen IA, Gnehm HP. Twelve-year follow-up after discontinuation of preseasonal grass pollen immunotherapy in childhood. Allergy. 2006; 61(2):198–201. 10.1111/j.1398-9995.2006.01011.x
24 Passalacqua G, Frati F, Puccinelli P, Scurati S, Incorvaia C, Canonica GW, et al. Adherence to sublingual immunotherapy: the allergists’ viewpoint. Allergy. 2009; 64(12):1796–7. 10.1111/j.1398-9995.2009.02136.x
25 Brüggenjürgen B, Reinhold T. Cost-effectiveness of grass pollen subcutaneous immunotherapy (SCIT) compared to sublingual immunotherapy (SLIT) and symptomatic treatment in Austria, Spain, and Switzerland. J Med Econ. 2018; 21(4):374–81. 10.1080/13696998.2017.1419959
26 Osterberg L, Blashke T. Adherence to medication. N Engl J Med. 2005; 353:487–93. 10.1056/NEJMra050100
27 Sabaté E. Adherence to long-term therapies: evidence for action. Switzerland: World Health Organization; 2003. World Health Organization. https://apps.who.int/iris/handle/10665/42682
28 Bidwal M, Lor K, Yu J, Ip E. Evaluation of asthma medication adherence rates and strategies to improve adherence in the underserved population at a Federally Qualified Health Center. Res Soc Adm Pharm. 2017; 13:759–66. 10.1016/j.sapharm.2016.07.007
29 Senna G, Caminati M, Lockey RF. Allergen immunotherapy adherence in the real world: how bad is it and how can it be improved? Curr Treat Options Allergy. 2015; 2:14. 10.1007/s40521-014-0037-6
30 Paoletti G, Di Bona D, Chu DK, Firinu D, Heffler E, Agache I, et al. Allergen immunotherapy: The growing role of observational and randomized trial “Real-World Evidence”. Allergy. 2021; 76(9):2663–72. 10.1111/all.14773
31 Di Bona D, Paoletti G, Chu DK, Pepys J, Macchia L, Heffler E, et al. Allergen immu-notherapy for respiratory allergy: Quality appraisal of observational comparative effectiveness studies using the REal Life Evidence AssessmeNt Tool. An EAACI methodology committee analysis. Clin Transl Allergy. 2021; 11(4):e12033. 10.1002/clt2.12033