
Download
ORIGINAL ARTICLE
A modified schedule of multiple aeroallergen ultra-rush immunotherapy in perennial allergic rhinitis: safety, efficacy, and T lymphocyte cell population studies
Nazila Ariaeea†, Ali Fouladvanda†, Mojgan Mohammadib, Reza Farid-Hosseinia, Amin Reza Nikpoorc, Maryam Khoshkhuia, Jalil Tavakkol-Afsharib, Farahzad Jabbari-Azada*
aAllergy Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
bImmunology Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
cMolecular Medicine Research Center, Hormozgan Health Institute, Hormozgan University of Medical Sciences, Bandar Abbas, Iran
†These being first authors contributed equally.
Abstract
Background: This study assessed whether a modified immunotherapy schedule for allergic rhinitis could be safe and efficient. Ultra-rush immunotherapy (URIT) rapidly desensitizes patients to aeroallergens.
Objective: We aimed to develop a modified URIT protocol in 3 days to achieve the target dose while observing whether it could improve this situation and decrease the time to achieve the maintenance dose.
Methods: The URIT was exercised in 21 patients with perennial allergic rhinitis. Premeditations were given to the patients 3 days prior to the immunotherapy and during the 3 days injections immunotherapy: pred nisolone, ranitidine, and Airokast/montelukast. Finally, the T cell population frequencies of patients prior to and after immunotherapy, including T helper 1, T helper 2, cytotoxic T lymphocytes, and regulatory T cells, were studied using flow cytometry. During the URIT protocol, 21 patients received 291 injections.
Result: Six patients (28.6%) showed systemic reactions in our study. All systemic reactions occurred on the third day by the 1:1 dilution of the maintenance dose. These systemic reactions occurred in three patients after 13 injections, and the three remaining patients showed systemic reactions following the last injection. No systemic reaction was observed on the first and second day of the therapy, and the risk of systemic reaction with every injection was about 2%. Among the T cell populations, CD3+ and CD8+ cells decreased significantly.
Conclusion: The findings emphasized that URIT, alongside premedication with a high dose of antihistamine, helped to achieve the maintenance dose and control clinical manifestations.
Key words: allergens, allergic rhinitis, immunotherapy, hypersensitivity
*Corresponding author: Farahzad Jabbari Azad, MD, Allergy Research Center, Qaem Hospital, Shariati Square, Mashhad, Iran. Email address: [email protected]
Received 20 November 2023; Accepted 1 April 2024; Available online 1 May 2024
Copyright: Ariaee N, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Allergic rhinitis causes several disorders, such as sleep disorders, weakness, depression, reduced attention, and impaired performance at work and school.1 It results in the loss of work and study performance, significantly impacting the quality of life of people suffering from this disease.2,3 The global prevalence of allergic rhinitis approximately 10–15%, of which 17–28% is in European countries.4 Also, the prevalence of allergic rhinitis in Iranian children and adults is about 18% and 25%, respectively.5
Allergic rhinitis can be a risk factor for exacerbating other diseases, such as asthma, sinusitis, and otitis media. It has also been found that between 15% and 38% of asthma patients have symptoms of allergic rhinitis. Moreover, expensive treatment of allergic rhinitis and its related disorders, such as asthma, sinusitis, and otitis media, are challenging issues for the healthcare system.4 Subcutaneous immunotherapy is a modern approach to allergic rhinitis. It has several benefits, including clinical decrease in disease period.6,7 However, routine subcutaneous immunotherapy protocols have several drawbacks that have led to the evaluation of different aspects of allergic rhinitis treatments to achieve the most apparent therapeutic results and safety.8
Several subcutaneous immunotherapy protocols, including a conventional protocol with weekly increasing doses to achieve optimum level within few months, are approved as an appropriate route of subcutaneous immunotherapy.9 Cluster protocol usually within 8 weeks reaches to optimum dose.10,11 Rush immunotherapy protocol allows eight injections in one day, then increasing the dose in 8–11 weeks to achieve optimum dose.12,13 On the other hand, ultra-rush immunotherapy (URIT) is used to obtain an effective dose within a short duration, and is effective in in the case of insect venom (wasps and bees); however, no reference is determined to use it in aeroallergens immunotherapy.14 Compared to conventional immunotherapies, rush immunotherapy and URIT have several priorities, such as reducing the time to achieve optimum dose in less than 1 week and reducing the production of allergen-specific immunoglobulin E (IgE) antibody, and the enhanced response of allergen-specific immunoglobulin G4 (IgG4) antibody. In addition, it is cost-effective because of reduced injection period.15
However, in spite of the benefits of rush immunotherapies, one of the biggest concerns related to these procedures is the occurrence of adverse systemic reactions. To address this drawback, administering premeditations prior to and during rush and ultra-rush immunotherapies could be effective.16,17 Therefore, the present study aimed to assess the clinical effectiveness of the mentioned immunotherapy and its generated immune responses reactions. Related adverse systemic reactions were also evaluated and compared with conventional immunotherapy.
Methods and Materials
Patients
The present clinical trial study was conducted from May 2015 to September 2016, comprising 21 patients with allergic rhinitis with an age range of 15–55 years from the immunology and allergy ward of Mashhad University of Medical Sciences, Mashhad, Iran. The patients were enrolled in the study after obtaining their written consent. The inclusion criteria of participants included clinical manifestations of allergic rhinitis, in which the prick skin test was positive by the prevalent commercial extracts of the region’s aeroallergens (Greer Laboratories, Lenoir, NC). The exclusion criteria from the study were uncontrolled asthma with forced expiratory volume 1 (FEV1) below 70% of the predicted value, remarkable cardiovascular diseases, usage of beta-blocker medications, insulin-dependent diabetes, autoimmune diseases, any history of previous anaphylactic shock, and dissatisfaction with participation and noncooperation in the study.
Study Design
This study was a prospective case series of a modified rush immunotherapy protocol to evaluate the efficacy, immunologic changes, and adverse events. All participants took the following premedication drugs started 3 days prior to the study and during 3 days of immunotherapy protocol: prednisolone 30 mg every 12 h, ranitidine 150 mg every 12 h, montelukast 10 mg once a day (OD), and telfast or fexofenadine 180 mg every 12 h. In order to assess the effects of premedication drugs or avoid using them by the patients, the histamine prick test was conducted by calculating the diameter of hives or swelling of the skin prior to the first injection of immunotherapy protocol. The demographic and clinical data and standard questionnaire of Sino-Nasal Outcome Test-22 (SNOT-22)16 and Mini Rhino Conjunctivitis Quality of Life Questionnaire (mini-RQLQ) of patients were recorded prior to the immunotherapy until 3 months after the intervention.17 The rush immunotherapy of patients based on was done using the following aeroallergens: (1) GS weed mix 1/20 w/v GP15AO3, (2) GS 7 grass mix 100.000 BAU/ML GTP27AO3, (3) GS 11 tree mix 1/20 w/v GPO714AO4, and (4) Salsola 1/20 w/v G59AO3.
Patients’ cardiopulmonary condition and local and systemic reactions were monitored during the injections until 1 h following the last injection. The systemic reactions were evaluated using the World Allergy Organization (WAO) guidelines.18 The patients were hospitalized up to 12 h following the last injection. Aerocast 10mg (Montelukast) and telfast 180 mg (Fexfenadin) were administered at least for 2 weeks, and prednisolone and ranitidine administrations were discontinued, following discharge from the hospital. Our protocol (Table 1) was modified based on the routine immunotherapy protocols. Immunotherapy was conducted by increasing the dose (adding 0.05 mg to the prevailing dose) of aeroallergens until attaining the optimum dose level. However, the rush immunotherapy was discontinued for patients with any sign of systemic reactions. The outpatient (after discharge) maintenance weekly therapy continued for 4 weeks and then every month.
Table 1 The modified rush-immunotherapy protocol timeline.
| Interval Time (h:min) | Dose (mL) | Dilution (v/v) |
|---|---|---|
| 1st Day | ||
| 00:00 | 0.05 | 1:10,000 |
| 15 min | 0.3 | 1:10,000 |
| 45 min | 0.1 | 1:1000 |
| 1 h 15 min | 0.3 | 1:1000 |
| 2 h 15 min | 0.1 | 1:100 |
| 3 h 15 min | 0.3 | 1:100 |
| 4 h 15 min | 0.1 | 1:10 |
| 5 h 15 min | 0.2 | 1:10 |
| 2nd Day | ||
| 00:00 | 0.2 | 1:10 |
| 1 h:00 min | 0.4 | 1:10 |
| 3 h 00 min | 0.05 | 1:1 |
| 3rd Day | ||
| 00:00 | 0.1 | 1:1 |
| 1 h 00 min | 0.3 | 1:1 |
| 3 h 00 min | 0.5 | 1:1 |
The time of initiation was considered 00:00.
Immunological assessment
To study immunological responses, 10 mL of ethylenediaminetetraacetic acid (EDTA) blood samples were collected from 15 randomly chosen patients. Intracellular and extracellular staining of peripheral blood mononuclear cells (PBMC) of the patient for flow cytometry analysis of the cytotoxic T lymphocyte (CTL [CD3+, CD8+, interferon gamma+, IFN-γ+]), T helper 1 (Th1 [CD3+, CD4+, IFN-γ+]), T helper 2 (Th2 [CD3+, CD4, interleukin 4+, IL-4+]), and T regulatory cells (CD4, CD25+, FoxP3+, and CD127-) were performed by BD FACS Calibur flow cytometry using True-Nuclear™ Transcription Factor Buffer Set (BioLegend®, San Diego, CA, USA) and the following antibodies: anti-human CD8 FITC (BioLegend®), anti-human CD4 FITC (BioLegend®, USA), anti-human CD25 PerCP-cyanine 5.5 (BioLegend®), anti-human CD127 APC (BioLegend®), anti-human CD3 PerCP-Cyanine 5.5 (BioLegend®), anti-human IFN-γ PE (BioLegend®), and anti-human IL-4 PE PerCP-Cyanine 5.5 (BioLegend®).
Statistical analysis
Descriptive statistics, paired T-test, one-way ANOVA, and post hoc tests were used with the SPSS software version 20. In addition, alternative nonparametric analyses of the above-mentioned statistical tests were considered. P < 0.05 was considered as statistically significant.
Results
Demographic data
In all, 21 patients, including 12 (57.1%) women and 9 (42.9%) men, with a mean age of 29.5 years, were included in the study. The clinical diagnosis of about 90% of the enrolled patients in the present study was allergic rhinitis (66%) and allergic rhinitis plus asthma (23.8%). According to the prick test results and clinical manifestations of patients, the most potential aeroallergens were selected, and the immunotherapy protocol was done on patients by the following aeroallergens: 19 (90.5%) by weed aeroallergen, 1 (4.5%) by grass aeroallergen, and 1 (4.5%) by tree aeroallergen. After 291 injections of aeroallergens, six patients showed manifestations of systemic reactions related to immunotherapy.
Table 2 presents the systemic reactions related to the immunotherapy, which occurred in six patients. During immunotherapy, no episode of cardiovascular arrest, hypotension, tachycardia, and anaphylactic shock was observed; systemic reactions were treated by antihistamines (four patients) and short-acting beta-agonists (SABA; two patients). One patient suffered from menstrual cramps. However, we wanted to ensure that no gastrointestinal (GI)-related anaphylaxis manifestations were observed; so, epinephrine was taken as a preventative measure for her.
Table 2 Clinical information of patients related to systemic reactions to immunotherapy.
| Reaction grade | Symptoms | Time to reaction | Dilution (v/v) | Number of Injections | Allergen | Epinephrine | SABA | H-1 |
|---|---|---|---|---|---|---|---|---|
| 1 | Urticaria | 6 h | 1/1 | 14 | Weed mix | No | No | Yes |
| 2 | Urticaria + SOB | 1 h | 1/1 | 14 | Weed mix | No | Yes | Yes |
| 1 | Urticaria | 2 h | 1/1 | 1 | Weed mix | No | No | Yes |
| 2 | Cough + uterine contraction | 30 min | 1/1 | 13 | Grass mix | Yes | No | No |
| 1 | SOB | 45 min | 1/1 | 13 | Salsola | No | Yes | No |
| 1 | Urticaria | 1 h | 1/1 | 13 | Tree mix | No | No | Yes |
SOB: shortness of breath; SABA: short-acting beta-agonists.
URIT affects clinical manifestations
The effects of URIT on clinical manifestations based on Mini-RQLQ and SNOT-22 questionnaires revealed that prior to and after the immunotherapy, the mean scores of SNOT-22 questionnaires were 45.2 ± 14.6 and 21.73 ± 18.67, respectively (P = 0.001). The mean scores of Mini-RQLQ questionnaire prior to and after the intervention were 35.66 ± 14.17 and 12.66 ± 10.03, respectively (P = 0.0001).
Role of URIT on immunological responses
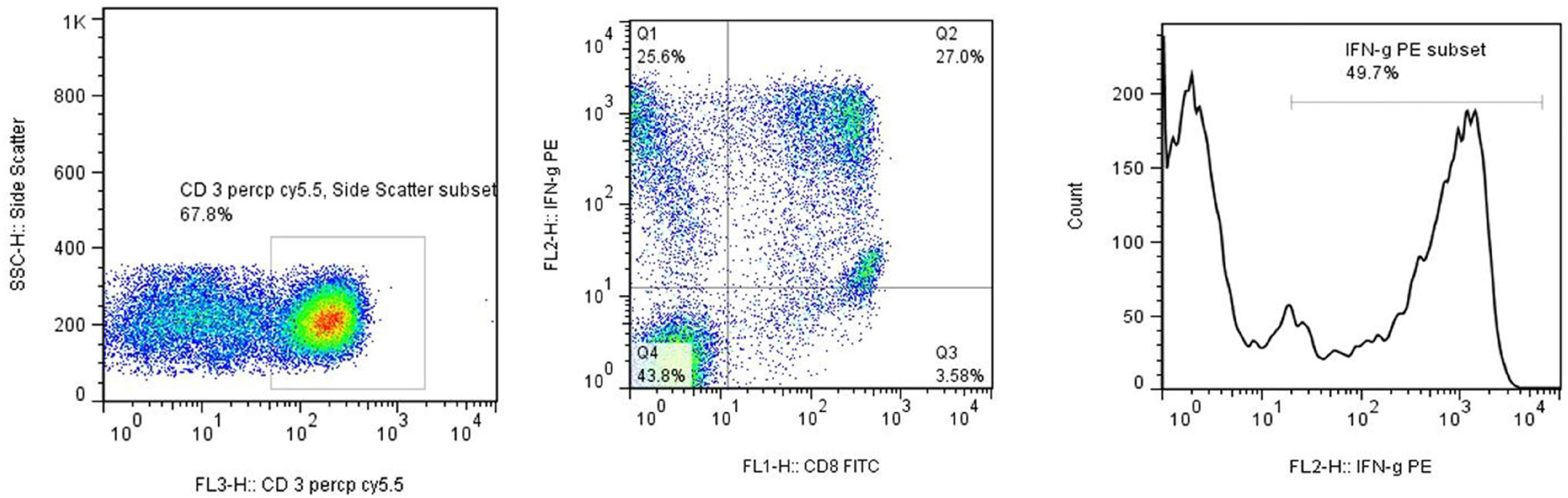
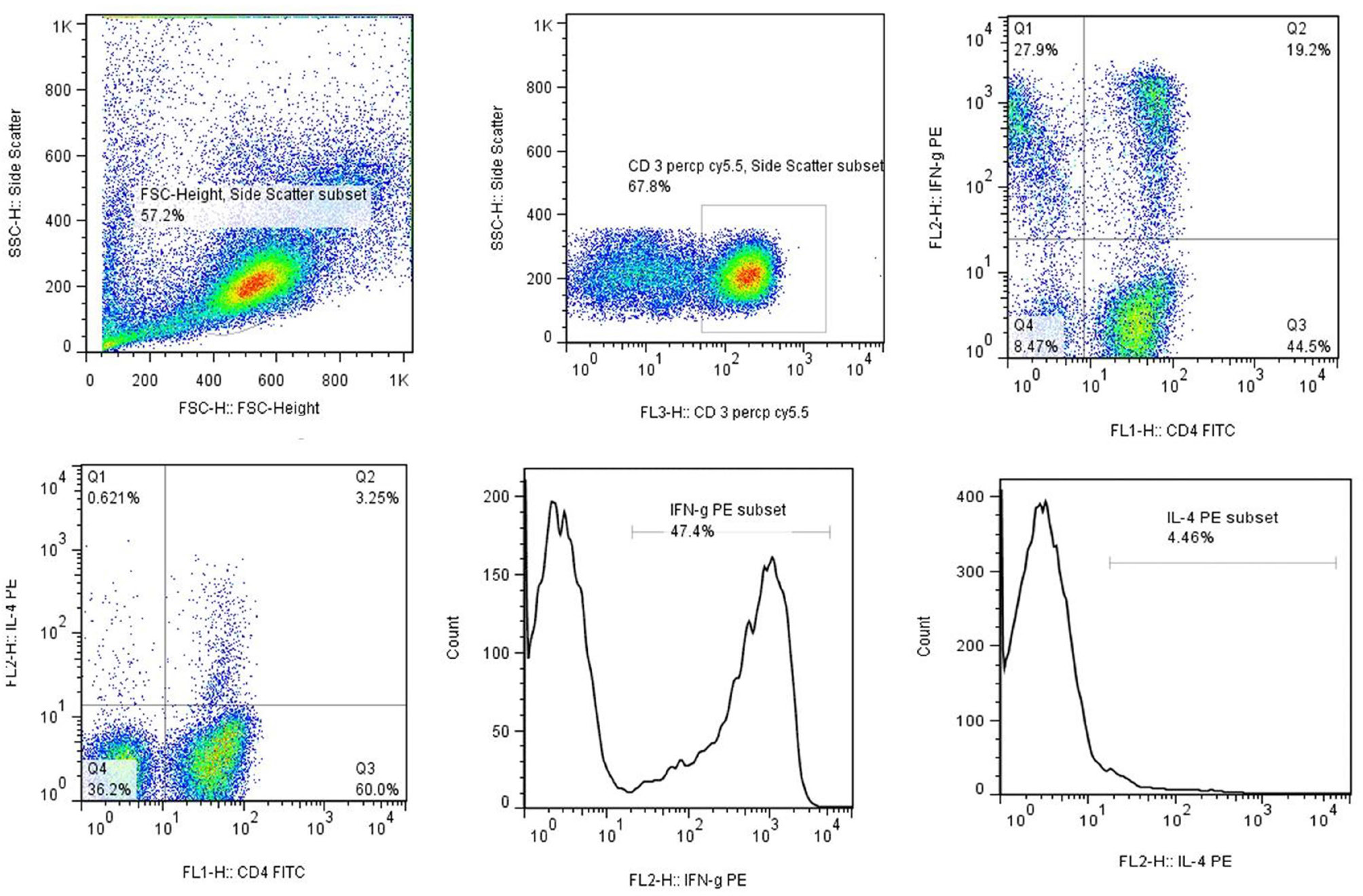
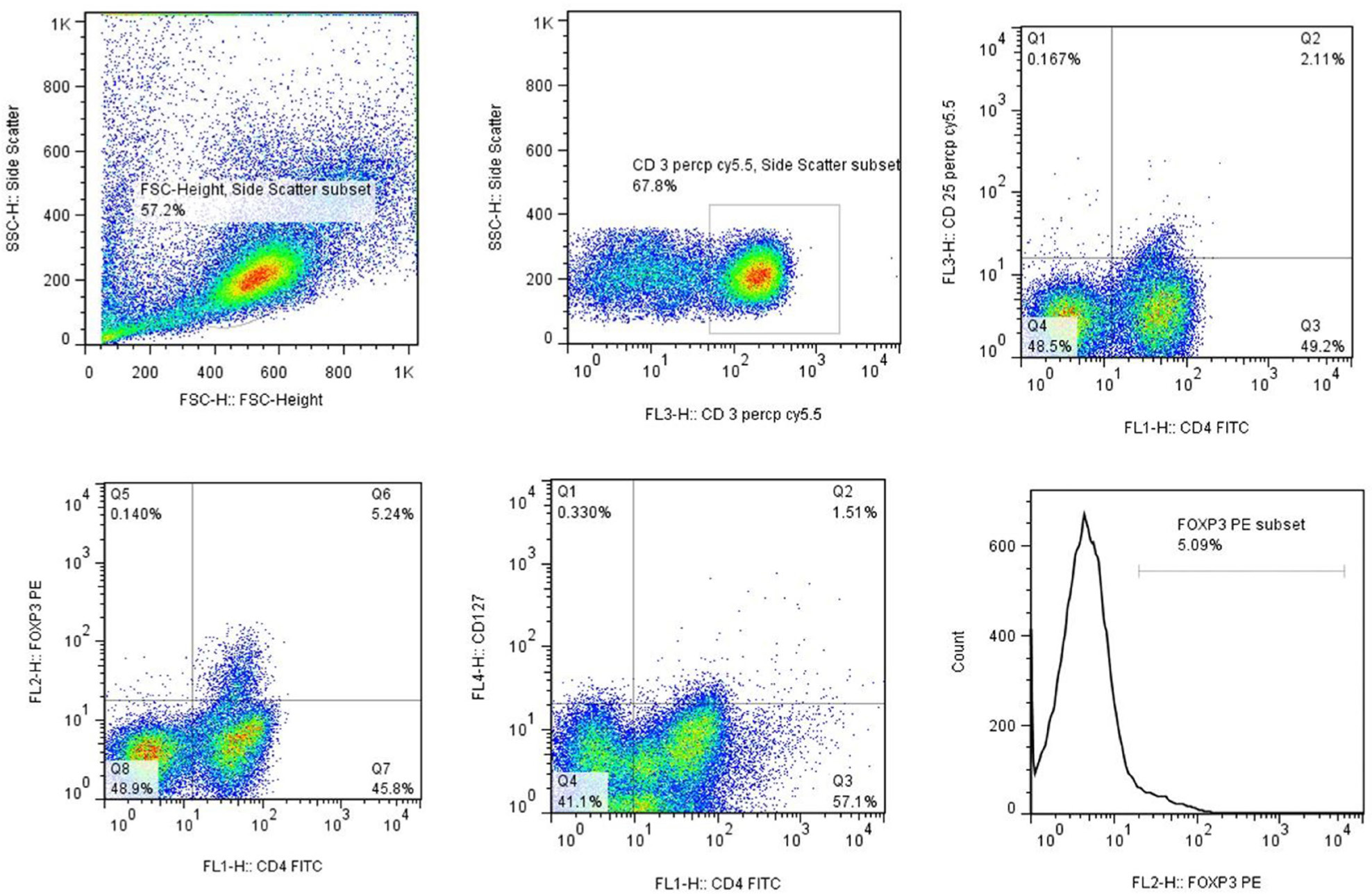
Figures 1–3 present the flow cytometry analysis of patients pre- and post-URIT. URIT effects in case of 15 patients were evaluated on immunological responses by measuring proportion of IL-4, IFN-γ cytokines, Th1, Th2, and T regulatory (Treg) cells by flow cytometry. The flow cytometry results are shown in Table 3.
Figure 1 Flow cytometry analysis of CD4+ T lymphocyte cells. The PBMC of patients were collected along with the intracellular and extracellular markers of CD4+ T lymphocyte cells (CD3+, CD4+, and IFN-g, or CD3+, CD4+, and IL-4+).
Figure 2 Flow cytometry analysis of CD8+ T lymphocyte cells. The PBMC of patients were collected along with the intracellular and extracellular markers of CD8+ T lymphocyte cells (CD3+, CD8+, and IFN-g+).
Figure 3 Flow cytometry analysis of regulatory T lymphocyte cells. The PBMC of patients were collected along with the intracellular and extracellular markers of regulatory T lymphocyte cells (CD4+, CD25+, Foxp3+, and CD127-).
Table 3 Immunological response profiles prior to and after ultra-rush immunotherapy.
| Before immunotherapy (mean±SD) | After immunotherapy (mean±SD) | P-value* | |
|---|---|---|---|
| IFN-γ MFI of CD3+ and CD4+-gated cells (Th1) | 179.21±123.62 | 246.50±127.28 | 0.164 |
| IFN-γ MFI of CD3+ and CD8+-gated cells (CTLs) | 103.35±54.48 | 102.91±80.84 | 0.983 |
| IL-4 MFI of CD3+ and CD4+-gated cells (Th2) | 20.22±10.95 | 24.69±14.03 | 0.514 |
| FoxP3 MFI of CD4+, CD25+, and CD127-gated cells (Th2) | 18.52±20.00 | 23.34±9.67 | 0.519 |
*Statistical analysis was done by Independent T-test.
The results indicated that post-URIT, CD8+ T cells (CTLs) reduced significantly (P = 0.032), while post-URIT, frequency of CD4+ T cells was not statistically significant. Moreover, frequency of Treg cells decreased following URIT, but the mentioned decrease was not statistically significant (P = 0.248). As shown in Table 4, alterations in other cell groups were not statistically significant (P > 0.05).
Table 4 Frequency of T lymphocyte subpopulations, pre- and post-ultra-rush immunotherapy data presented as mean percentage ± SD.
| Cell populations | Before immunotherapy | After immunotherapy | P-value* |
|---|---|---|---|
| CD3+ and CD8+ cells | 37.46±8.86 | 33.26±8.65 | 0.032 |
| CD3+ and CD4+ cells | 49.26±5.39 | 51.90±5.53 | 0.320 |
| CD4+, CD25+, Foxp3+, and CD127 cells (Treg) | 1.25±0.79 | 0.94±0.39 | 0.248 |
| CD3+, CD4+, and IL-4+ cells (Th2) | 1.54±0.49 | 2.06±0.69 | 0.059 |
| CD3+ CD4+ IFN-γ+ cells (Th1) | 11.40±4.41 | 11.56±5.38 | 0.923 |
| CD3+, CD4+, and CD8+ cells (CTL) | 23.19±7.27 | 24.01±6.97 | 0.607 |
*Statistical analysis was done by Independent T-test.
Discussion
The present study was conducted to evaluate the effectiveness of a modified URIT and its generated immune responses and the related systemic adverse reactions, compared to the routine immunotherapy used for allergic rhinitis.18
Our hypothesis was to reduce the time to attain maintenance dose to relieve symptoms sooner and convince the patients to continue with the therapy. Thus, a modified rush immunotherapy protocol was prepared to achieve a monthly maintenance dose. This protocol replaced the weekly build-up plan after the rush immunotherapy, and the patients attained the maintenance dose on the third day of the therapy. The purpose in this study was to assess the immunity level and immune responses of patients with allergic rhinitis after using new immunotherapy method, which to our knowledge was carried out for the first time in the clinic. Systemic reactions through this protocol were 28.6%, almost similar to the literature,18,19 which reported 20–33% systemic reactions. However, Cox et al. reported more systemic reactions in immunotherapy with inhaled allergens (in 27–100% of patients after rush immunotherapy and 0–79% of patients post cluster immunotherapy).20,21 In a rush immunotherapy study, systemic reactions were observed in 38% of patients.22 Bousquet et al. reported that 34.4% of dust mite-sensitive, allergic asthma patients demonstrated systemic reactions after rush immunotherapy.23 In all the above-mentioned studies, the rush immunotherapy protocol was achieved in 1 day (equivalent to the first day of our protocol), followed by a weekly build-up plan for attaining the maintenance dose.
Immunotherapy procedures reduce the activity of mast cells and basophils, such as cytokine secretion, mast cell priming by antigen-specific IgE antibodies, and degranulation of the granules containing allergy-induced components. This selective suppression is affected by alterations in different immune system parameters, including reducing allergen-specific IgE levels and specific Treg cells frequency. Suppression of high-affinity IgE receptor, FcɛRI, activates basophils with selective suppression of H2 receptor-mediated histamine, and release of sulfide-leukotrienes (LTs) could be associated with fast induction of allergen tolerance and desensitization effect, particularly in venom immunotherapy.24
Histamines are a low molecular weight monoamine components that bind to four different G-protein receptors with different effects on immune responses. Released histamine induces peripheral tolerance by several mechanisms. Stimulation of H1 receptors enhances Th1 responses,25 because CD4+ Th1 cells express H1 receptors in themselves.26 Because of different effects of histamines on immune responses via H1 and H2 receptors, injecting a high dose of allergens in URIT could release high amounts of histamines. However, the low frequency of systemic effects in our study could be due to the high dose of administered antihistamine, compared to the results of previous studies, in which suppression of H1 receptors stopped the production of histamines by basophils and mast cells.27
The systemic reactions that occurred during premedication could be due to some unknown mechanisms, hence precautions must be taken. Our study’s 3-month clinical results were similar to conventional subcutaneous immunotherapy, which was done by Dolz et al.28 In order to evaluate immune responses after rush immunotherapy, a study was conducted by Lack et al. involving 10 children with asthma, allergic to dust mites.29 It showed that after 2–4 weeks of rush immunotherapy, 1–2 days after attaining the maintenance dose, the allergen-specific IgE and IgG4 were reduced and T helper cells proliferation was suppressed, but the frequency of CD8+ cytotoxic T cells was increased.29 In the present study, induction of CTL frequency was observed, although not statistically significant (P > 0.05). Specific IgE and IgG4 were not evaluated in our study. Since the level of specific IgE and IgG4 can be induced by immunotherapy, evaluating specific IgE and IgG4 is strongly recommended for future studies.
In our study, the evaluation of immune responses and changes in clinical manifestation were monitored up to 3 months after the maintenance dose, which may not be a convenient time to observe changes in immune responses. We suggest studying various time points post-immunotherapy. The limitation of our study was the lack of control groups for conventional and rush immunotherapy in order to compare results. Therefore, amelioration in patients was compared with their first-day conditions prior to URIT.
Different unknown mechanisms may be involved in the induction of tolerance by the rapid protocols of immunotherapy, such as rush immunotherapy and URIT, which are different from conventional immunotherapy. It is obvious that with a bigger sample size, normalization of patients and standardized assays of immunological responses could obtain the exact effect of URIT.
Conclusion
The present study showed that URIT, combined with premeditations and continuing taking an antihistamine –Leukotriene inhibitor daily for 2 weeks after the rash phase could help lessen clinical manifestations. In our study, the timing and number of allergens injected to induce systemic reaction were not similar to previous studies. The reactions in our study were at much higher doses than in previous studies. Therefore, URIT with premeditations could be a candidate for optimal immunotherapy to treat allergic rhinitis, particularly for patients to whom advanced health facilities are unavailable.
Ethics approval and consent to participate
The study was approved by the Ethical Committee of Mashhad University of Medical Sciences (IR.MUMS.fm.REC.1394.362) and trial registration: Iranian Registry of Clinical Trials, IRCT2017010123235N8; Registered: 25 June 2017; retrospectively registered at: https://www.irct.ir/trial/19853.
Availability of data and materials
The datasets generated and analyzed during the current study are not available publicly because of patients’ data and ethical issues, but are available from the corresponding author on reasonable request.
Competing interests
The authors declared that they had no competing interests.
Funding
The study was financially supported by the Mashhad University of Medical Sciences (Grant No.: 940678).
Author contributions
Ali Fouladvand, Reza Farid Hosseini, Maryam Khoshkhui, and Farahzad Jabbari carried out treatments, selected patients, and followed. Nazila Ariaee, Mojgan Mohammadi, Amin Reza Nikpoor, and Jalil Tavakkol-Afshari performed immunological examinations. Nazila Ariaee analyzed data and designed the project. All authors read critically and approved the final manuscript.
Acknowledgments
The authors thanked Maral Amini for her collaboration.
REFERENCES
1. Ariaee N, Panahi M, Bakhshaee M, Ghorbani J, Ravanshad Y, Hosseini RF, et al. Shirazi thyme (Zataria multiflora) extract can alleviate allergic rhinitis: A randomized clinical trial. Adv Dermatol Allergol (Postępy Dermatologii i Alergologii). 2021;38(3):520–5. 10.5114/ada.2020.102295
2. Long AA. Findings from a 1000-patient internet-based survey assessing the impact of morning symptoms on individuals with allergic rhinitis. Clin Ther. 2007;29(2):342–51. 10.1016/j.clinthera.2007.02.007
3. Meltzer EO, Blaiss MS, Derebery MJ, Mahr TA, Gordon BR, Sheth KK, et al. Burden of allergic rhinitis: Results from the pediatric allergies in America survey. J Allergy Clin Immunol. 2009;124(3):S43–70. 10.1016/j.jaci.2009.05.013
4. Brożek JL, Bousquet J, Baena-Cagnani CE, Bonini S, Canonica GW, Casale TB, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines: 2010 Revision. J Allergy Clin Immunol. 2010;126(3):466–76. 10.1016/j.jaci.2010.06.047
5. Kalmarzi RN, Ataee P, Fathollahpour A, Behzadifar M, Moradi M, Sharifian F, et al. The prevalence of allergic rhinitis among iranian children: A systematic review and meta--analysis. Endocr Metab Immune Disord Drug Targets. 2020;20(2):189–97. 10.2174/1871530319666190515100735
6. Eng P, Borer-Reinhold M, Heijnen I, Gnehm H. Twelve-year follow-up after discontinuation of preseasonal grass pollen immunotherapy in childhood. Allergy. 2006;61(2):198–201. 10.1111/j.1398-9995.2006.01011.x
7. Pajno G, Barberio G, De Luca F, Morabito L, Parmiani S. Prevention of new sensitizations in asthmatic children monosensitized to house dust mite by specific immunotherapy. A six-year follow-up study. Clin Exp Allergy. 2001;31(9):1392–7. 10.1046/j.1365-2222.2001.01161.x
8. Hoseini RF, Jabbari F, Rezaee A, Rafatpanah H, Yousefzadeh H, Ariaee N, Sadri H. House dust mite sublingual-swallow immunotherapy in perennial rhinitis: A double-blind, placebo-controlled Iranian study. J Biol Regul Homeost Agents. 2018;32(1):83–8.
9. Padró C, Gutiérrez D, Moreno F, Parra A, Rial MJ, Lleonart R, et al. Effectiveness and safety of a microcrystalline tyrosine-adjuvanted Dermatophagoides pteronyssinus allergoid immunotherapy in adult patients with allergic asthma and rhinitis: A real-life prospective observational study. Immun Inflamm Dis. 2022;10(5):e585. 10.1002/iid3.585
10. Greiwe J, Bernstein JA (Editors). Accelerated/rush allergen immunotherapy. Allergy Asthma Proc. 2022. 10.2500/aap.2022.43.210108
11. Mauro M, Russello M, Alesina R, Sillano V, Alessandrini A, Dama A, et al. Safety and pharmacoeconomics of a cluster administration of mite immunotherapy compared to the traditional one. Eur Ann Allergy Clin Immunol. 2006;38(1):31–4.
12. Van Mason J, Portnoy JM. Accelerated immunotherapy: Why are we going so slow? Curr Treat Options Allergy. 2019;6:396–409. 10.1007/s40521-019-00212-3
13. Weitzer T, Mueller R. The safety of rush immunotherapy in the management of canine atopic dermatitis—230 cases. Vet Dermatol. 2023. 10.1111/vde.13170
14. Brown SG, Wiese MD, Van Eeden P, Stone SF, Chuter CL, Gunner J, et al. Ultrarush versus semirush initiation of insect venom immunotherapy: A randomized controlled trial. J Allergy Clin Immunol. 2012;130(1):162–8. 10.1016/j.jaci.2012.02.022
15. Temiño VM, Wu P, Konig J, Fahrenholz JM (Editors). Safety of multiple aeroallergen rush immunotherapy using a modified schedule. Allergy Asthma Proc. 2013. 10.2500/aap.2013.34.3651
16. Chu CH, Caldwell JW, Cristiano LM, Petrov AA, Traister RS. Safety of a modified environmental rush immunotherapy protocol in the pediatric population. Ann Allergy Asthma Immunol. ,2022;128(5):600–1. 10.1016/j.anai.2021.12.011
17. Nelson HS. Injection immunotherapy for inhalant allergens. In: Middleton’s allergy. Cambridge, MA: Elsevier; 2014, pp. 1416–37. 10.1016/B978-0-323-08593-9.00088-7
18. Smits WL, Giese JK, Letz KL, Inglefield JT, Schlie AR, editors. Safety of rush immunotherapy using a modified schedule: A cumulative experience of 893 patients receiving multiple aeroallergens. Allergy Asthma Proc. 2007. 10.2500/aap.2007.28.2996
19. Cox L, Calderon MA. Subcutaneous specific immunotherapy for seasonal allergic rhinitis: A review of treatment practices in the US and Europe. Curr Med Res Opin. 2010;26(12):2723–33. 10.1185/03007995.2010.528647
20. Cox L. Accelerated immunotherapy schedules: Review of efficacy and safety. Ann Allergy Asthma Immunol. 2006;97(2):126–38. 10.1016/S1081-1206(10)60003-8
21. Cox L, Larenas-Linnemann D, Lockey RF, Passalacqua G. Speaking the same language: The World Allergy Organization subcutaneous immunotherapy systemic reaction grading system. J Allergy Clin Immunol. 2010;125(3):569–74. e7. 10.1016/j.jaci.2009.10.060
22. Harvey SM, Laurie S, Hilton K, Khan DA. Safety of rush immunotherapy to multiple aeroallergens in an adult population. Ann Allergy Asthma Immunol. 2004;92(4):414–9. 10.1016/S1081-1206(10)61776-0
23. Bousquet J, Hejjaoui A, Dhivert H, Clauzel A, Michel F. Immunotherapy with a standardized dermatophagoides pteronyssinus extract: III. Systemic reactions during the rush protocol in patients suffering from asthma. J Allergy Clin Immunol. 1989;83(4):797–802. 10.1016/0091-6749(89)90017-1
24. Nelson HS. The evolution of allergy immunotherapy. Ann Allergy Asthma Immunol. 2021;126(4):357–66. 10.1016/j.anai.2020.11.011
25. Mandola A, Nozawa A, Eiwegger T. Histamine, histamine receptors, and anti-histamines in the context of allergic responses. Lympho Sign J. 2019;6(2):35–51. 10.14785/lymphosign-2018-0016
26. Meghnem D, Oldford SA, Haidl ID, Barrett L, Marshall JS. Histamine receptor 2 blockade selectively impacts B and T cells in healthy subjects. Sci Rep. 2021;11(1):9405. 10.1038/s41598-021-88829-w
27. Oettgen HC. Mast cells in food allergy: Inducing immediate reactions and shaping long-term immunity. J Allergy Clin Immunol. 2022. 10.1016/j.jaci.2022.10.003
28. Dolz I, Martinez-Cocera C, Bartolome J, Cimarra M. A double-blind, placebo-controlled study of immunotherapy with grass-pollen extract Alutard SQ during a 3-year period with initial rush immunotherapy. Allergy. 1996;51(7):489–500. 10.1111/j.1398-9995.1996.tb04655.x
29. Lack G, Nelson HS, Amran D, Oshiba A, Jung T, Bradley KL, et al. Rush immunotherapy results in allergen-specific alterations in lymphocyte function and interferon-γ production in CD4+ T cells. J Allergy Clin Immunol. 1997;99(4):530–8. 10.1016/S0091-6749(97)70081-2