
Download
ORIGINAL ARTICLE
Evaluation of treatment and long-term management of anaphylaxis in pediatric departments of Greece: a 2-year nationwide survey
Evanthia Chiampoua*, Konstantinos Dourosb, Dafni Morikib, Mitrogiorgou Marinab, Anastasia Anastasiou-Katsiardanic, Kalliopi Tanouc, Vasilis Grammeniatisd, Anna Zisid, Evanthia Perikleousd, Emmanouil Galanakise, Marilia Lioudakie, Fotini Vrouvakie, Soultana Kolyvaf, Antigoni Mavroudig, Maria Nivatsih, Stergianna Ntoumai, Evangelia Stefanakij, Maria Trigak, Panagiota Kakavak, Olga Lagiouk, Kostas N. Priftisb, Nikolaos Chaliasosl, Sophia Tsabouril
aDepartment of Pediatrics, University Hospital of Ioannina, Ioannina, Greece
bPediatric Allergy and Respiratory Unit, 3rd Department of Pediatrics, “Attikon” University Hospital, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece
cDepartment of Paediatrics, Achillopouleio General Hospital of Volos, Volos, Thessaly, Greece
dDepartment of Paediatrics, General Hospital of Ioannina, Ioannina, Greece
eDepartment of Paediatrics, University Hospital, University of Crete, Heraklion, Crete, Greece
fDepartment of Paediatrics, General Hospital of Chania, Crete, Heraklion, Greece
g3rd Pediatric Department, Hippokration Hospital, Aristotle University of Thessaloniki, Thessaloniki, Greece
hPediatric Department, Hippokration Hospital, Aristotle University of Thessaloniki, Thessaloniki, Greece
i2nd Department of Pediatrics, AHEPA University General Hospital of Thessaloniki, Aristotle University of Thessaloniki, Thessaloniki, Greece
jDepartment of Pediatrics, Venizeleion General Hospital, Heraklion, Crete, Greece
kPediatric Allergy Unit, Department of Pediatrics, University Hospital of Patras, Rion, Patras, Greece
lChild Health Department, University of Ioannina School of Medicine, Ioannina, Greece
Abstract
Background: Anaphylaxis proportions of incidence are increasing globally. However, limited data are available regarding anaphylaxis in the pediatric population of Greece.
Purpose: The aim of the study was to evaluate management of anaphylaxis in Greek pediatric departments.
Methods: We performed a questionnaire-based study of children aged less than 16 years presenting with anaphylaxis in 10 national pediatric hospitals over a period of 2 years. Management of anaphylaxis was assessed prior to and after an informative intervention.
Results: In all, 127 cases of anaphylaxis were identified. Epinephrine was administered in almost half of all cases (51.2%), predominantly through intramuscular route (88.5%), while the majority of anaphylaxis patients were treated with antihistamines (92.9%) and corticosteroids (70.1%). Epinephrine was more likely administered by physicians if the elicitor was a drug (P < 0.003). Regarding long-term management, an epinephrine auto-injector was prescribed in 66.9% of patients. Follow-up information was available for most of the patients (92.9%), the majority of whom (76.3%) were referred to an allergist. More than half of these patients (63.6%) had a documented allergy follow-up, which identified a causative allergen in 53.3% of cases. No statistically significant differences were recorded prior to and after the intervention regarding management of anaphylaxis.
Conclusions: This nationwide study highlighted the necessity of further improvement in terms of anaphylaxis treatment and secondary prevention measures. This presupposes appropriate education and training of healthcare professionals, thus contributing to proper and comprehensive care of the pediatric population.
Key words: acute treatment, anaphylaxis, children, epinephrine, long-term management
*Corresponding author: Evanthia Chiampou, Department of Pediatrics, University Hospital of Ioannina, Ioannina, Greece. Email address: [email protected]
Received 5 November 2023; Accepted 6 March 2024; Available online 1 May 2024
Copyright: Peñaranda A, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Anaphylaxis incidence rate is increasing globally and is considered as the most severe end of the spectrum of allergic reactions, is defined as an acute, rapidly progressive hypersensitivity reaction derived from the massive release of inflammatory mediators from mast cells and basophils after exposure to an allergy-causing substance. Since severe anaphylaxis is characterized by potentially lethal airway and/or circulation compromise even in the absence of typical skin features, it is imperative that it is promptly recognized and managed by all healthcare professionals.1–3
Although it is difficult to estimate precisely the incidence of anaphylaxis, a worldwide systematic epidemiological review focusing on children has shown highly variable proportions, ranging from 1 to 761 per 100,000 person-years for total anaphylaxis, and from 1 to 77 per 100,000 person-years for food-induced anaphylaxis. Certainly, the global incidence data cannot be integrated to the Greek pediatric population for which respective data are lacking. However, recent data have indicated a global increase in both emergency department (ED) visits and hospitalizations because of anaphylaxis over the past two decades, particularly in the pediatric population.
As a growing public health issue, it is crucial for ED physicians to be familiar with the diagnosis and management of this clinical emergency entity.4–11 However, there are barriers regarding timely identification and proper management of anaphylaxis. Until recently, the lack of internationally accepted definition and diagnostic criteria, combined with the lack of reliable laboratory biomarkers for confirmation of diagnosis, has resulted in underdiagnosis and, therefore, undertreatment of anaphylaxis. Moreover, a wide variability in clinical presentation, especially in the absence of cutaneous clinical manifestations, makes the diagnosis of anaphylaxis challenging for healthcare professionals. The recognition and management of anaphylaxis is even more challenging in the pediatric population, particularly in infants, because of their inability to accurately describe clinical manifestations as well as atypical and nonspecific manifestations, such as crying, irritability, or lethargy.12–15
Intramuscular (IM) administration of epinephrine is the cornerstone of anaphylaxis treatment and must be administered without delay, even in suspicion of impending anaphylaxis, as it prevents progression of anaphylactic reaction and reduces mortality, hospitalization rate, and the likelihood of biphasic reactions.1,2,16–20
Long-term management is of paramount importance in every patient who has experienced anaphylaxis. Implementation of measures to prevent and effectively treat possible future adverse reactions should include prescription of an epinephrine auto-injector (EAI), patient education, and referral to an allergist for identification of suspected trigger, prevention of recurrences, and allergen immunotherapy (AIT) if indicated.3,21,22 Despite international guidelines, however, several studies have documented that both acute and long-term management of anaphylaxis remains inadequate.23–26
The present study aimed to assess the management practices of anaphylaxis applied at Greek pediatric hospital departments in accordance with the current guidelines. Our primary objective was to identify deficiencies in diagnosis and management of anaphylactic episodes, and to evaluate whether any improvement was recorded to the above variables after an informative intervention was conducted. Secondary objective was to increase awareness of national guidelines in terms of diagnosis and appropriate management of anaphylaxis among healthcare professionals in Greece, thus contributing to the proper and comprehensive care of the pediatric population of the country.
Materials and Methods
We performed a questionnaire-based study of all children aged < 16 years who presented to Greek pediatric hospital departments with clinical manifestations of anaphylaxis during a 2-year period (May 2019–May 2021). Ten secondary and tertiary care hospitals across the country accepted to participate in this registry by reporting all patients diagnosed with anaphylaxis at their EDs.
Questionnaires were prepared based on the guidelines of the World Allergy Organization for the assessment and management of anaphylaxis27 and administered to the participating departments. Subsequently, pediatricians were asked to complete this questionnaire during the patient’s first visit in ED or hospitalization.
The questionnaire covered demographic data (age and gender), atopic status of the child, family history of atopy, previous anaphylactic reactions, clinical signs and symptoms, suspected trigger mentioned by the patient (or relatives) and the pediatric ED physician, and pre-hospital and ED management. The severity of anaphylaxis was defined according to the Ring and Messmer classification.28 Patients were followed up 2 months after the acute episode regarding the long-term management of anaphylaxis, such as EAI prescription, their referral to an allergist, and the identification of trigger for anaphylactic episode.
The study was structured as follows: For a 10-month period, pediatric ED physicians recorded the anaphylaxis cases presenting in pediatric hospital departments, using Questionnaire A (stage 1). Then, during one-day meeting with the pediatricians of the participating departments, the two authors presented the data collected at stage 1 and discussed about the difficulties or concerns that occurred during collection of the data. At the same time, the participants were informed of the current international guidelines regarding diagnosis, treatment, and long-term management of anaphylaxis in the pediatric population (stage 2–intervention). Finally, the recording of anaphylaxis cases continued for 12 more months, using a similar questionnaire, that is, Questionnaire B (stage 3).
Children that attended pediatric ED and presented anaphylaxis for more than one occasion during the study period were counted as different cases because causative agents and clinical manifestation could vary from one episode to another.
The statistical analysis was performed using the SPSS v26.0 software. Frequencies and percentage values were used within the context of the study to describe all recorded categorical data. The Pearson’s chi square test was used to test all hypotheses, while Fisher’s exact test was applied to all cases with the assumption that regarded the expected minimum numbers per cell and the expected number of cells with a frequency of less than 5 was not met. A multiple logistic regression model was used to assess the effect of different variables on administration of epinephrine in patients presenting with anaphylaxis; P < 0.05 was considered statistically significant.
Results
During the study period, 127 cases of anaphylaxis were recorded in 125 children (65 cases prior to and 62 cases after the informative intervention). Patients’ characteristics, elicitors, and involvement of the organ system are summarized in Table 1.
Table 1: Characteristics of all children diagnosed with anaphylaxis
| N (%) of children | |
|---|---|
| Gender | |
| Male | 82 (64.5%) |
| Female | 45 (35.4%) |
| Age range (years) | |
| 0–2 | 34 (26.8%) |
| 3–5 | 27 (21.3%) |
| 6–11 | 45 (35.4%) |
| >12 | 21 (16.5%) |
| History of atopic disease | 82 (64.56%) |
| Food allergy | 51 (62.2%) |
| Atopic dermatitis | 44 (53.65%) |
| Allergic rhinitis | 17 (17.07%) |
| Asthma | 7 (8.54%) |
| Other allergies | 6 (7.32%) |
| Family history of atopy | 68 (53.54%) |
| Elicitors | |
| Food | 70 (55.11%) |
| Drugs | 18 (14.17%) |
| Insect venom | 16 (12.6%) |
| AIT | 7 (5.51%) |
| Others | 8 (6.3%) |
| Unknown | 8 (6.3%) |
| Organ system involved | |
| Skin | 116 (91.34%) |
| Gastrointestinal tract | 62 (48.82%) |
| Respiratory tract | 86 (67.72%) |
| Cardiovascular tract | 19 (14.96%) |
| More than 2 systems involved | 38 (30.16%) |
| Severity grade | |
| Grade 2 | 116 (91.3%) |
| Grade 3 | 10 (7.9%) |
| Grade 4 | 1 (0.8%) |
*Others: food-dependent, exercise-induced anaphylaxis, cold, exercise.
AIT: allergen immunotherapy.
Grade 2: mild to moderate symptoms; Grade 3: severe pulmonary, cardiovascular, and/or gastrointestinal symptoms; Grade 4: cardiac or respiratory arrest.
Pre-hospital treatment
On arrival at EDs, 49 out of 127 (38.9%) children had already received treatment. Among the patients who had received pre-ED treatment, the majority had received corticosteroids (75.5%) and antihistamines (73.5%). Approximately one out of four patients had received both corticosteroids and antihistamines. Adrenaline was used in 36.7% (18/49) of the patients. For the majority (89%) of the patients treated with epinephrine prior to their arrival at EDs, the drug was administered by a healthcare professional and only 11% of the patients had received treatment through a self-injectable EAI. In all, 7.8% patients had received pre-hospital treatment with epinephrine, corticosteroids, and antihistamines concurrently.
Acute management
Regarding the ED treatment, epinephrine was administered in more than half of the anaphylaxis cases (51.2%). Comparing pre-intervention period to post-intervention period, no significant difference was observed in administration of epinephrine (P = 0.652).
Most of the patients (88.5%) received epinephrine predominantly through the IM route. IM route of administration was used by most of pediatric ED physicians during post-intervention period, although without statistical significance (P = 0.369). Other routes of administration were subcutaneous, intravenous bolus, and inhalation via nebulization.
Most of the patients (90%) received a single dose of epinephrine and only six out of 127 (10%) patients were treated with more than one dose of adrenaline by ED physicians. During the post-intervention period, the commonest reason for not using epinephrine by caregivers was mild clinical symptoms (76.2%), followed by the uncertainty that the episode was anaphylactic (9.52%), fear of adverse reactions (9.52%), and hesitation regarding correct dosage and route of administration (4.76%).
The associated factors for epinephrine administration in patients presented with anaphylaxis are given in Table 2. Multivariate logistic regression showed that drugs as elicitors could be a significant factor associated with the greater possibility of epinephrine administration.
Table 2: Multiple logistic regression analysis for the effect of intervention, elicitor factors, and severity regarding administration of epinephrine in patients presenting with anaphylaxis, adjusting for gender, age, and history of atopy.
| B | SE | Wald | df | Significance | OR | 95% CI for OR | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Gender | 985 | 631 | 2436 | 1 | 119 | 373 | 108 | 1287 |
| Age | 2834 | 3 | 418 | |||||
| 3–5 years vs 0–2 years | -494 | 809 | 372 | 1 | 542 | 610 | 125 | 2981 |
| 6–11 years vs 0–2 years | -1336 | 815 | 2688 | 1 | 101 | 263 | 053 | 1298 |
| 12+ years vs 0–2 years | -768 | 1010 | 579 | 1 | 447 | 464 | 064 | 3356 |
| Atopy history | 507 | 615 | 679 | 1 | 410 | 1660 | 497 | 5537 |
| Intervention (before vs after) | 850 | 605 | 1974 | 1 | 160 | 2340 | 715 | 7657 |
| Elicitor factor | 10,576 | 7 | 158 | |||||
| Drug | 2982 | 996 | 8964 | 1 | 003 | 19,728 | 2801 | 138,967 |
| Insect venom | 811 | 877 | 854 | 1 | 355 | 2249 | 403 | 12543 |
| Uknown | 1892 | 1299 | 2123 | 1 | 145 | 6632 | 520 | 84,530 |
| AIT | 1231 | 1520 | 656 | 1 | 418 | 3425 | 174 | 67,417 |
| Others | 1054 | 1942 | 295 | 1 | 587 | 2871 | 064 | 129,051 |
| Constant | -2890 | 824 | 12,302 | 1 | 000 | 056 | ||
OR: odds ratio; 95% CI: 95% confidence interval.
The vast majority of patients received acute treatment with antihistamines (118/127) and corticosteroids (89/127); however, no significant difference was discovered for both medications between pre- and post-intervention periods. A smaller proportion of patients received treatment with inhaled beta-2 agonists (22.8%), oxygen therapy (7.9%), and intravenous fluids (18.1%) without statistical difference between pre- and post-intervention periods. The treatment prior to and after the intervention is summarized in Table 3.
Table 3: Acute anaphylaxis treatment prior to and after intervention.
| Acute treatment | Total | Intervention | P-value | |||
|---|---|---|---|---|---|---|
| Before | After | |||||
| N | Ν | % | Ν | % | ||
| Epinephrine | 65 | 32 | 49.2% | 33 | 53.2% | 0.652 |
| Antihistamines | 118 | 63 | 96.9% | 55 | 88.7% | 0.071 |
| Corticosteroids | 89 | 45 | 69.2% | 44 | 70.9% | 0.831 |
Almost all patients (98%) remained in the hospital for observation for at least 24 h. No biphasic or protracted reaction was recorded. One fatality (0.7%) was recorded during the study period. A 6-year-old girl with an immunoglobulin E (IgE)-mediated cow’s milk allergy developed anaphylactic shock at school after she accidentally consumed pastry with butter. No EAI was available and the girl was transferred to hospital; however, the rescue team could not save her.
Long-term management
At discharge, 85 patients (66.9%) received an EAI prescription, eight of whom already had an EAI. This proportion was almost similar between the two study periods. All the patients in the study had received instructions for the correct use of EAI during the two study periods.
Follow-up
Follow-up information was available for 118 of 127 (92.9%) patients in the study. In less than half of these patients (46.6%), follow-up care was arranged as an outpatient, with the majority of them (79.5%) showing up and being reassessed by a primary care physician in the following days after the episode. Follow-up care was arranged for a smaller proportion of patients during the post-intervention period, although with no statistical difference between the two study periods (P = 0.168).
Allergist referral
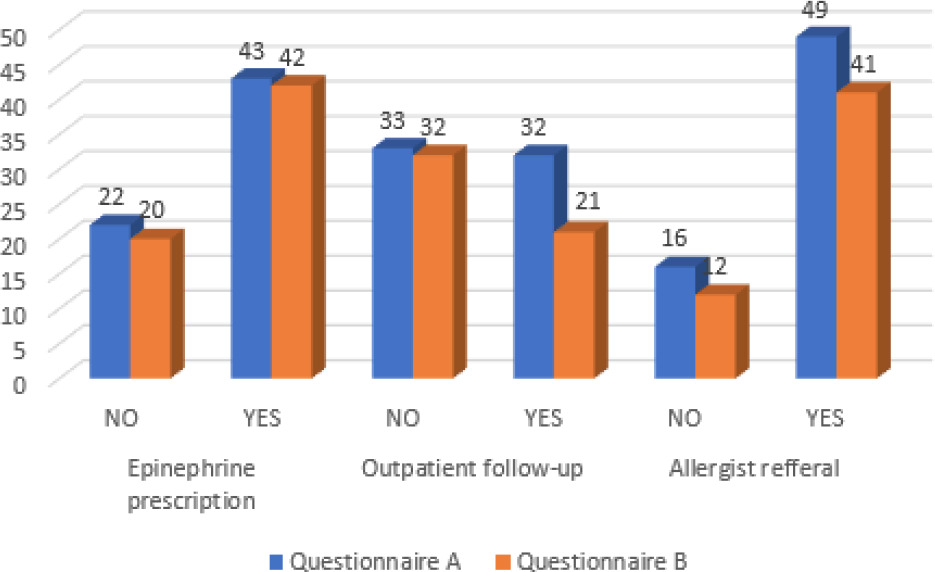
Among patients with follow-up information, three out of four (76.3%) patients were referred to an allergist, with similar proportion of referrals between the two study periods (P = 0.802) (Figure 1) and 63.6% had a documented allergy assessment, including measurement of specific serum IgE and skin prick test during subsequent months. Fewer than 12% patients were assessed by an allergist during the post-intervention period, although without statistical difference (P = 0.156). Among the patients who underwent allergy testing, only 40 (53.3%) had a certain causative agent identified. Finally, the initially suspected trigger coincided with the trigger after the allergy follow-up in 38 of the 40 patients (95%). Long-term management, prior to and after the intervention, is summarized in Table 4 and Figure 1.
Figure 1: Long-term management of patients diagnosed with anaphylaxis prior to (questionnaire A: blue bar) and after (questionnaire B: orange bar) the informative intervention.
Table 4: Long-term management of anaphylaxis prior to and after intervention.
| Long-term management |
Total | Intervention | P-value | |||
|---|---|---|---|---|---|---|
| Before | After | |||||
| N | Ν | % | Ν | % | ||
| Epinephrine prescription | 85 | 43 | 66.1% | 42 | 67.7% | 0.849 |
| Outpatient follow-up | 55 | 32 | 49.2% | 23 | 37.1% | 0.168 |
| Allergist referral | 90 | 49 | 75.4% | 41 | 77.4% | 0.802 |
| Allergy assessment | 75 | 45 | 69.2% | 30 | 56.6% | 0.156 |
Discussion
To our knowledge, this was the first nationwide multicenter study that provided insight into the treatment and long-term management of children presenting with anaphylaxis in the pediatric departments of Greece hospitals.
Although all patients in our study met the National Institute of Allergy and Infectious Disease and the Food Allergy and Anaphylaxis Network criteria for anaphylaxis,1 almost half of them (48.8%) did not receive epinephrine as first-line treatment, which is in contrast to all current guidelines. The patients that did not receive epinephrine had resolution of clinical manifestations by the time they had arrived the EDs.
Varying proportions of administration of epinephrine globally were reported by different studies. This could be attributed to various reasons, such as different educational programs for healthcare providers among countries, different management protocols at EDs as well as different study designs and methods. Data from the European Anaphylaxis Register for a 10-year period showed that only 27.1% of patients with anaphylaxis were treated with epinephrine by caregivers, with Greece ranking first in terms of proportion of epinephrine administration (66.7%). The higher proportions reported in Greece could be attributed to the fact that the data derived from a pediatric department, with qualified medical personnel, of the largest referral center for children with allergies in Greece. On the contrary, our study included 10 secondary and tertiary care pediatric hospitals, rather than specialized allergy centers.29–31 Contrary to the above-mentioned data, retrospectively reviewed anaphylaxis cases presented in an ED of a Melbourne hospital in Australia, and found that epinephrine was administered to the majority (95%) of children with anaphylaxis.
The present study discovered that the main reason for underuse of epinephrine, as reported by healthcare professionals, was that on arrival to ED, the symptoms had lessened, and therefore administration of epinephrine was not considered. Moreover, treatment with epinephrine suffered because of uncertainty regarding anaphylaxis episode, hesitation concerning appropriate dose and route of administration as well as fear of possible associated adverse effects. These findings were not singular to our study, as several studies reported the same reasons regarding underutilization of epinephrine by healthcare professionals.32–35
The underutilization of epinephrine in ED settings could be partially attributed to the challenge in diagnosing anaphylaxis because of heterogeneity in clinical presentation as well as variability in definitions and diagnostic criteria. Diagnosis could be challenging if the episode was the first anaphylactic reaction, the elicitor was not known, and the cutaneous symptoms were absent. Moreover, the underuse of epinephrine in anaphylaxis could be related to lack of knowledge or compliance to anaphylaxis guidelines. Finally, lack of ongoing education to healthcare providers as well as lack of standard management protocols in pediatric ED contributes to suboptimal management of anaphylaxis.
It is interesting to note that after our informative intervention, a slight increase in epinephrine administration (from 49.23% to 53.22%) was observed, although it was not of statistical significance. Underutilization of epinephrine could be partly attributed to the lack of standard management protocols in the pediatric ED in Greek hospitals. On the contrary, a study conducted by Arroabarren et al. in a Spanish pediatric ED showed significant increase in epinephrine administration after implementation of an anaphylaxis protocol (from 27% to 57.6%; P = 0.012).36 Therefore, establishment of standardized anaphylaxis protocol in EDs is crucial, as it could substantially increase utilization of epinephrine.
It was encouraging to observe in our study that the majority of patients received epinephrine via IM route, considered to be the superior route, as it achieved higher and more rapid peak plasma concentrations and was associated with lower risk of overdose and cardiovascular complications.37–39 Comparable high proportions of IM administration were also reported in other studies.40,41 The high proportion of IM route of administration could be related to the qualified personnel managing anaphylaxis patients in tertiary care hospitals, as observed in the participating departments of our study. However, no significant difference was discovered between pre- and post-intervention groups regarding the route of epinephrine administration.
When compared to other elicitors, intake of drugs was a significant factor associated with greater possibility of epinephrine administration. This could be explained by the fact that drugs are associated with more severe reactions in general, and with refractory anaphylaxis (anaphylaxis reaction with persistence of symptoms despite treatment with at least two doses of IM epinephrine) in particular.42,43 In addition, according to the studies conducted in Europe and the United States, although uncommon, drugs account for most of anaphylaxis fatalities not only in adults but also in the pediatric population.44–46
Moreover, antihistamines and corticosteroids were administered more frequently than epinephrine for managing acute anaphylaxis in the participating pediatric EDs. Our results substantiated the results of other studies that demonstrated a consistently high usage of antihistamines and corticosteroids for managing anaphylaxis.40,47,48 It was worth noting that there was no statistically significant difference in administration of antihistamines and corticosteroids prior to and after our intervention. A possible explanation for the reported higher use of antihistamines was the fact that the majority of anaphylactic episodes in our study was accompanied by cutaneous symptoms; moreover, based on other studies, antihistamines are useful in relieving manifestations such as urticaria and pruritus.49–51 On the other hand, use of corticosteroids for managing anaphylaxis could be attributed to their anti-inflammatory action, particularly in patients exhibiting bronchospasm or the upper airway edema. Additionally, it is a common belief, although without any evidence, that corticosteroids could reduce the risk of biphasic and protracted anaphylaxis.52–54
According to the studies, an estimated 1% of hospitalization and 0.1% of ED admissions for anaphylaxis resulted in fatal outcomes. However, mortality in the present study was lower compared to the literature.55
EAI prescription in our study was found to be relatively higher, compared to previous studies.56–59 However, no significant difference was observed about EAI use between pre- and post-intervention periods. Underutilization of EAI could be partly attributed to the fact that some patients who had experienced prior anaphylaxis were using EAI and therefore no further prescription was required. Additionally, although the guidelines suggest an EAI of 0.15 mg for infants weighing >7.5 kg, many physicians avoided prescribing it to this age group, probably because of fear of dose-related adverse effects.60 All patients in the present study had received instructions for the correct use of EAI prior to discharged from hospital.
The reported proportion of follow-up in outpatient clinics after discharge was low and became lower during the post-intervention period, although no statistical difference was found between the two study periods. A possible explanation for this, and especially during the post-intervention period, could be the COVID-19 pandemic, which affected patients’ referrals because of stricter regulations, as outpatient clinics were cancelled for several months to minimize the risk of contagion.
Several studies reported that the COVID-19 pandemic had a direct impact on the healthcare system, leading to a decline in the quality of medical care. In many countries, a significant decrease in outpatient visits to clinics during the COVID-19 lockdown period was noted because of fear of exposure to coronavirus disease, leading to worsening of health conditions. Similarly, a study conducted by Arsenault et al. discovered that during the COVID-19 pandemic, a decrease of 9–40% was observed in outpatient visits in 10 different countries.61–64
Contrary to multiple studies demonstrating low proportion of allergist referrals after an anaphylactic episode,39,57–59 our results showed a high proportion of patients being referred to an allergist for further management, although without any statistical difference between the two study periods.
However, the proportion of patients that underwent an allergy follow-up left a lot to be desired, although the allocation was greater compared to other studies.65,66 The patients’ suboptimal adherence to post-discharge instructions could be due to misunderstanding or underestimation of the importance of allergy assessment in minimizing the risk of recurrence. Additionally, the lower proportion of post-intervention allergy assessment could be due to the COVID-19 pandemic, leading to delay or even avoidance of medical care.
Anaphylaxis is a growing public health issue, and given the life-threatening nature of the reaction, there is an urgent need to increase and update knowledge among healthcare professionals regarding its acute treatment, the EAI prescription, and the patient’s referral to an allergist for follow-up. First, it is imperative for healthcare providers to stay complaint with the international guidelines to minimize underdiagnosis and undertreatment of anaphylaxis. Continuous medical education is required to increase awareness about management of anaphylaxis among health professionals. This can be achieved through training programs comprising clinical scenarios and simulation training, series of lectures, or e-learning courses. Moreover, studies in pediatric ED show a significant increase in epinephrine administration after implementation of anaphylaxis protocol. Therefore, in order to upgrade the level of anaphylaxis management, it is highly recommended to establish anaphylaxis protocol in EDs in the form of a written emergency plan, including drugs and dosages. It is known that anaphylaxis patients are most frequently attended by primary healthcare providers, rather than allergists. Finally, it is important to create a close collaboration between ED physicians and allergy specialists, with the latter disseminating knowledge to other healthcare providers for the proper management of patients with anaphylaxis.
One of the strengths of our study was the prospective, multi-center data collection of pediatric patients presenting with anaphylaxis to participating departments of Greece. However, the present study had a series of limitations. First, our population was a small sample size, which could have affected the results. Moreover, participation in the study was voluntary and was based on clinicians’ interest to engage the registry. In addition, the study included only patients who gave written consent to participate, and, therefore, we cannot rule out that some patients refused to participate. Another limitation could be the possibility of under-reporting of cases and incomplete data recording, which could have lead to missing of information. Although this is a multi-center study with participation of 10 pediatric departments from all over the country, the limited number of patients included in the study, along with the voluntary participation of healthcare providers and patients, does not allow generalization of the results.
Conclusion
This nationwide study affirmed the current literature regarding suboptimal management practices in children diagnosed with anaphylaxis in pediatric EDs in Greece. Acute management of anaphylactic episodes fell short of expectations, as epinephrine was underutilized and the second-line treatments, such as antihistamines and corticosteroids, were overutilized. However, there were satisfactory proportions of EAI prescriptions at discharge and the majority of our patients were referred to an allergist for further assessment. Despite internationally established guidelines, knowledge gaps in the diagnosis and treatment of anaphylaxis impede the effective management of patients with anaphylaxis. Thus, we stress upon the need for ongoing education and frequent practical training programs for healthcare professionals and the adoption of standardized written plans for managing anaphylaxis in EDs. We also highlight the crucial role of allergists in increasing awareness by educating pediatricians and other healthcare providers, aiming the proper and comprehensive care of the pediatric population suffering with anaphylaxis.
REFERENCES
1. Sampson HA, Muñoz-Furlong A, Campbell RL, Adkinson NF Jr, Bock SA, Branum A, et al. Second symposium on the definition and management of anaphylaxis: Summary report–Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network Symposium. J Allergy Clin Immunol. 2006 Feb;117(2):391–7.
2. Fischer D, Vander Leek TK., Ellis, AK, Kim H. Anaphylaxis. Allergy Asthma Clin Immunol. 2018 Sep 12;14(Suppl 2):54. 10.1186/s13223-018-0283-4
3. Cardona V, Ansotegui IJ, Ebisawa M, El-Gamal Y, Fernandez Rivas M, Fineman S, et al. World Allergy Organization Anaphylaxis Guidance 2020. World Allergy Organ J. 2020 Oct 30;13(10):100472. 10.1016/j.waojou.2020.100472
4. Wang Y, Allen KJ, Suaini NHA, McWilliam V, Peters RL, Koplin JJ. The global incidence and prevalence of anaphylaxis in children in the general population: A systematic review. Allergy. 2019 Jun;74(6):1063–80. 10.1111/all.13732
5. Motosue MS, Bellolio MF, Van Houten HK, Shah ND, Campbell RL. National trends in emergency department visits and hospitalizations for food-induced anaphylaxis in US children. Pediatr Allergy Immunol. 2018 Aug;29(5):538–44. 10.1111/pai.12908
6. Conrado AB, Ierodiakonou D, Gowland MH, Boyle RB, Turner PJ. Food anaphylaxis in the United Kingdom: Analysis of national data, 1998–2018. Br Med J (BMJ). 2021 Feb 17;372:n251. 10.1136/bmj.n251
7. Nocerino R, Leone L, Cosenza L, Berni Canani R. Increasing rate of hospitalizations for food-induced anaphylaxis in Italian children: An analysis of the Italian Ministry of Health database. J Allergy Clin Immunol. 2015 Mar;135(3):833–5.e3. 10.1016/j.jaci.2014.12.1912
8. Pyrpyris N, Kritikou M, Aggelidis X, Manolaraki I, Makris M, Papadopoulos NG, Xepapadaki P. Anaphylaxis in children and adolescents: Greek data analysis from the European Anaphylaxis Registry (NORA). J Pers Med. 2022 Sep 30;12(10):1614. 10.3390/jpm12101614
9. Mullins RJ, Dear KB, Tang ML. Time trends in Australian hospital anaphylaxis admissions in 1998–1999 to 2011–2012. J Allergy Clin Immunol. 2015 Aug;136(2):367–75. 10.1016/j.jaci.2015.05.009
10. Tejedor Alonso MA, Moro Moro M, Múgica García MV. Epidemiology of anaphylaxis. Clin Exp Allergy. 2015 Jun;45(6):1027–39. 10.1111/cea.12418
11. Michelson KA, Monuteaux MC, Neuman MI. Variation and trends in anaphylaxis care in United States children’s hospitals. Acad Emerg Med. 2016 May;23(5):623–7. 10.1111/acem.12922
12. Quoc QL, Bich TCT, Jang JH, Park HS. Recent update on the management of anaphylaxis. Clin Exp Emerg Med. 2021 Sep;8(3):160–72. 10.15441/ceem.21.121
13. Sclar DA, Lieberman PL. Anaphylaxis: Underdiagnosed, underreported, and undertreated. Am J Med. 2014 Jan;127(1 Suppl):S1–5. 10.1016/j.amjmed.2013.09.007
14. Dribin TE, Motosue MS, Campbell RL. Overview of allergy and anaphylaxis. Emerg Med Clin North Am. 2022 Feb;40(1):1–17. 10.1016/j.emc.2021.08.007
15. Shroba JA. Infant anaphylaxis: Diagnostic and treatment challenges. J Am Assoc Nurse Pract. 2020 Feb;32(2):176–83. 10.1097/JXX.0000000000000386
16. Australasian Society of Clinical Immunology and Allergy (ASCIA). Guidelines for the acute management of anaphylaxis. Accessed 19 April 2021.
17. Kim H, Fischer D. Anaphylaxis. All Asth Clin Immun. 2011;7(Suppl 1):S6. 10.1186/1710-1492-7-S1-S6
18. Fleming JT, Clark S, Camargo CA Jr, Rudders SA. Early treatment of food induced anaphylaxis with epinephrine is associated with a lower risk of hospitalization. J Allergy Clin Immunol Pract. 2015 Jan–Feb;3(1):57–62. 10.1016/j.jaip.2014.07.004
19. Alqurashi W, Stiell I, Chan K, Neto G, Alsadoon A, Wells G. Epidemiology and clinical predictors of biphasic reactions in children with anaphylaxis. Ann Allergy Asthma Immunol. 2015 Sep;115(3):217–23.e2. 10.1016/j.anai.2015.05.013
20. Ellis AK. Priority role of epinephrine in anaphylaxis further underscored—The impact on biphasic anaphylaxis. Ann Allergy Asthma Immunol. 2015 Sep;115(3):165. 10.1016/j.anai.2015.06.024
21. Simons FE. Anaphylaxis. J Allergy Clin Immunol. 2010 Feb;125 (Suppl 2):S161–81. 10.1016/j.jaci.2009.12.981
22. Simons FE. Anaphylaxis, killer allergy: Long-term management in the community. J Allergy Clin Immunol. 2006 Feb;117(2):367–77. 10.1016/j.jaci.2005.12.002
23. Fineman SM, Bowman SH, Campbell RL, Dowling P, O’Rourke D, Russell WC, et al. Addressing barriers to emergency anaphylaxis care: From emergency medical services to emergency department to outpatient follow-up. Ann Allergy Asthma Immunol. 2015 Oct;115(4):301–5. 10.1016/j.anai.2015.07.008
24. Russell WS, Farrar JR, Nowak R, Hays DP, Scmitz N, Wood J, et al. Evaluating the management of anaphylaxis in US emergency departments: Guidelines vs. practice. World J Emerg Med. 2013;4(2):98–106. 10.5847/wjem.j.issn.1920-8642.2013.02.003
25. Robinson M, Greenhawt M, Stukus DR. Factors associated with epinephrine administration for anaphylaxis in children before arrival to the emergency department. Ann Allergy Asthma Immunol. 2017 Aug;119(2):164–9. 10.1016/j.anai.2017.06.001
26. Sidhu N, Jones S, Perry T, Thompson T, Storm E, Melguizo Castro AS, et al. Evaluation of anaphylaxis management in a pediatric emergency department. Pediatr Emerg Care. 2016 Aug;32(8):508–13. 10.1097/PEC.0000000000000864
27. Simons FE, Ardusso LR, Bilo MB, El-Gamal YM, Ledford DK, Ring J, et al. World Allergy Organization guidelines for the assessment and management of anaphylaxis. World Allergy Organ J. 2011 Feb;4(2):13–37. 10.1097/WOX.0b013e318211496c
28. Ring J, Messmer K. Incidence and severity of anaphylactoid reactions to colloid volume substitutes. Lancet.1977 Feb 26;1(8009):466–9. 10.1016/S0140-6736(77)91953-5
29. Grabenhenrich LB, Dölle S, Ruëff F, Renaudin JM, Scherer K, Pföhler C, et al. Epinephrine in severe allergic reactions: The European anaphylaxis register. J Allergy Clin Immunol Pract. 2018 Nov–Dec;6(6):1898–906.e1. 10.1016/j.jaip.2018.02.026
30. Gaspar Â, Santos N, Faria E, Pereira AM, Gomes E, Câmara R, et al. Anaphylaxis in children and adolescents: The Portuguese Anaphylaxis Registry. Pediatr Allergy Immunol. 2021 Aug;32(6):1278–86. 10.1111/pai.13511
31. Rangkakulnuwat P, Sutham K, Lao-Araya M. Anaphylaxis: Ten-year retrospective study from a tertiary-care hospital in Asia. Asian Pac J Allergy Immunol. 2020 Mar;38(1):31–9.
32. Pouessel G, Antoine M, Pierache A, Dubos F, Lejeune S, Deschildre A. Pediatric Emergency Medicine Group. Factors associated with the underuse of adrenaline in children with anaphylaxis. Clin Exp Allergy. 2021 May 51(5):726–9. 10.1111/cea.13821
33. Prince BT, Mikhail I, Stukus DR. Underuse of epinephrine for the treatment of anaphylaxis: Missed opportunities. J Asthma Allergy. 2018 Jun 20;11:143–51. 10.2147/JAA.S159400
34. Anagnostou K, Turner PJ. Myths, facts and controversies in the diagnosis and management of anaphylaxis. Arch Dis Child. 2019 Jan;104(1):83–90. 10.1136/archdischild-2018-314867
35. Simon FE, Clark S, Camargo CA Jr. Anaphylaxis in the community: Learning from the survivors. J Allergy Clin Immunol. 2009 Aug;124(2):301–6. 10.1016/j.jaci.2009.03.050
36. Arroabarren E, Lasa EM, Olaciregui I, Sarasqueta C, Muñoz JA, Pérez-Yarza EG. Improving anaphylaxis management in a pediatric emergency department. Pediatr Allergy Immunol. 2011 Nov;22(7):708–14. 10.1111/j.1399-3038.2011.01181.x
37. Simons FE, Gu X, Simons KJ. Epinephrine absorption in adults: Intramuscular versus subcutaneous injection. J Allergy Clin Immunol. 2001 Nov;108(5):871–3. 10.1067/mai.2001.119409
38. Campbell RL, Bellolio MF, Knutson BD, Bellamkonda VR, Fedko MG, Nestler DM, et al. Epinephrine in anaphylaxis: Higher risk of cardiovascular complications and overdose after administration of intravenous bolus epinephrine compared with intramuscular epinephrine. J Allergy Clin Immunol. 2015 Jan–Feb;3(1):76–80. 10.1016/j.jaip.2014.06.007
39. Simons FE, Roberts JR, Gu X, Simons KJ. Epinephrine absorption in children with a history of anaphylaxis. J Allergy Clin Immunol.1998 Jan;101(Pt 1):33–7. 10.1016/S0091-6749(98)70190-3
40. Vera MJ, Tagaro IC. Anaphylaxis diagnosis and management in the emergency department of a tertiary hospital in the Philippines. Asia Pac Allergy. 2020 Jan 13;10(1):e1. 10.5415/apallergy.2020.10.e1
41. Jeong K, Ye YM, Kim SH, Kim KW, Kim JH, Kwon JW, et al. A multicenter anaphylaxis registry in Korea: Clinical characteristics and acute treatment details from infants to older adults. World Allergy Organ J. 2020 Aug 11;13(8):100449. 10.1016/j.waojou.2020.100449
42. Francuzik W, Dölle-Bierke S, Knop M, Scherer Hofmeier K, Cichocka-Jarosz E, García BE, et al. Refractory anaphylaxis: Data from the European anaphylaxis registry. Front Immunol. 2019 Oct 18;10:2482. 10.3389/fimmu.2019.02482
43. Pouessel G, Deschildre A, Dribin TE, Ansotegui IJ, Cardona V, Chinthrajah RS, et al. Refractory anaphylaxis: A new entity for severe anaphylaxis. J Allergy Clin Immunol Pract. 2023 Jul;11(7):2043–8. 10.1016/j.jaip.2023.04.037
44. Pouessel G, Tanno LK, Claverie C, Lejeune S, Labreuche J, Dorkenoo A, et al. Fatal anaphylaxis in children in France: Analysis of national data. Pediatr Allergy Immunol. 2018 Feb;29(1):101–4. 10.1111/pai.12828
45. Jerschow E, Lin RY, Scaperotti MM, McGinn AP. Fatal anaphylaxis in the United States, 1999–2010: Temporal patterns and demographic associations. J Allergy Clin Immunol. 2014 Dec;134(6):1318–28.e7. 10.1016/j.jaci.2014.08.018
46. Cardinale F, Amato D, Mastrototaro MF, Caffarelli C, Crisafulli G, Franceschini F, et al. Drug-induced anaphylaxis in children. Acta Biomed. 2019 Jan 30;90(3-S):30–5.
47. Ezzat MHM, Shousha GAH, Gabal HAMS, Mousa MM. Anaphylaxis in children: Experience of an Egyptian center. Int J Allergy Asthma (IJAA). 2021;107. 10.29011/IJAA-107.100007
48. Jiang N, Xu W, Xiang L. Age-related differences in characteristics of anaphylaxis in Chinese children from infancy to adolescence. World Allergy Organ J. 2021 Nov 18;14(11):100605. 10.1016/j.waojou.2021.100605
49. Shaker MS, Wallace DV, Golden DBK, Oppenheimer J, Bernstein JA, Campbell RL, et al. Anaphylaxis—A 2020 practice parameter update, systematic review, and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) analysis. J Allergy Clin Immunol. 2020 Apr;145(4):1082–123. 10.1016/j.jaci.2020.01.017
50. Muraro A, Worm M, Alviani C, Cardona V, Dunn Galvin A, Garvey LH, et al. European Academy of Allergy, Clinical Immunology Food Allergy, Anaphylaxis Guidelines Group. EAACI guideline: Anaphylaxis (2021 update). Allergy. 2022 Feb 77(2):357–77. 10.1111/all.15032
51. Nurmatov UB, Rhatigan E, Simons FER, Sheikh A. H2 antihistamines for the treatment of anaphylaxis with and without shock: A systematic review. Ann Allergy Asthma Immunol. 2014 Feb;112(2):126–31. 10.1016/j.anai.2013.11.010
52. Auth RD, Zheng T, Berk J. Things We Do for No Reason™: Routine use of corticosteroids for the treatment of anaphylaxis. J Hosp Med. 2022 Mar;17(3):211–4. 10.12788/jhm.3665
53. Alqurashi W, Ellis AK. Do corticosteroids prevent biphasic anaphylaxis? J Allergy Clin Immunol Pract. 2017 Sep–Oct;5(5):1194–205. 10.1016/j.jaip.2017.05.022
54. Campbell DE. Australia. Anaphylaxis management: Time to re-evaluate the role of corticosteroids. J Allergy Clin Immunol Pract. 2019 Sep–Oct;7(7):2239–40. 10.1016/j.jaip.2019.07.005
55. Turner PJ, Jerschow E, Umasunthar T, Lin R, Campbell DE, Boyle RJ. Fatal anaphylaxis: Mortality rate and risk factors. J Allergy Clin Immunol Pract. 2017 Sep–Oct;5(5):1169–78. 10.1016/j.jaip.2017.06.031
56. Gabrielli S, Clarke A, Morris J, Eisman H, Gravel J, Enarson P, et al. Evaluation of pre-hospital management in a Canadian emergency department anaphylaxis cohort. J Allergy Clin Immunol Pract. 2019 Sep–Oct;7(7):2232–8.e3.10.1016/j.jaip.2019.04.018
57. Alvarez-Perea A, Ameiro B, Morales C, Zambrano G, Rodríguez A, Guzmán M, et al. Anaphylaxis in the pediatric emergency department: Analysis of 133 cases After an allergy workup. J Allergy Clin Immunol Pract. 2017 Sep–Oct;5(5):1256–63.10.1016/j.jaip.2017.02.011
58. Tritt A, Gabrielli S, Zahabi S, Clarke A, Moisan J, Eisman H, et al. Long-term management of cases of venom-induced anaphylaxis is suboptimal. Ann Allergy Asthma Immunol. 2018 Aug;121(2):229–34.e1 10.1016/j.anai.2018.04.006
59. Burnell FJ, Keijzers G, Smith P. Review article: Quality of follow-up care for anaphylaxis in the emergency department. Emerg Med Australas. 2015 Oct;27(5):387–93. 10.1111/1742-6723.12458
60. Muraro A, Worm M, Alviani C, Cardona V, DunnGalvin A, Garvey LH, et al. European Academy of Allergy and Clinical Immunology, Food Allergy, Anaphylaxis Guidelines Group. EAACI guidelines: Anaphylaxis (2021 update). Allergy. 2022 Feb 77(2):357–77. 10.1111/all.15032
61. Ahmead M, Daghlas F. The effect of the COVID-19 pandemic on the provision of outpatient clinic services in East Jerusalem hospitals: Patients’ perspectives. Front Public Health. 2023 Nov 24;11:1252449. 10.3389/fpubh.2023.1252449
62. Singh K, Xin Y, Xiao Y, Quan J, Kim D, Nguyen TPL, et al. Impact of the COVID-19 pandemic on chronic disease care in India, China, Hong Kong, Korea, and Vietnam. Asia Pacific J Public Health. 2022;34:392–400. 10.1177/10105395211073052
63. Noncommunicable Diseases, Rehabilitation and Disability (NCD). The impact of the COVID-19 pandemic on noncommunicable disease resources and services: Results of a rapid assessment. Geneva, Switzerland: World Health Organization (WHO); 2020. Available from: https://apps.who.int/iris/handle/10665/334136 (Accessed: December 29, 2021).
64. Arsenault C, Gage A, Kim MK, Kapoor NR, Akweongo P, Amponsah F, et al. COVID-19 and resilience of healthcare-systems in ten countries. Nat Med. 2022;28:1314–24. 10.1038/s41591-022-01750-1
65. Campbell RL Park MA, Kueber Jr MA, Lee S, Hagan JB. Outcomes of allergy/immunology follow-up after an emergency department evaluation for anaphylaxis. J Allergy Clin Immunol Pract. 2015 Jan–Feb;3(1):88–93. 10.1016/j.jaip.2014.07.011
66. Landsman-Blumberg PB, Wei W, Douglas D, Smith DM, Clark S, Camargo Jr CA. Food-induced anaphylaxis among commercially insured US adults: Patient concordance with post-discharge care guidelines. J Allergy Clin Immunol Pract. 2013 Nov–Dec;1(6):595–601.e1. 10.1016/j.jaip.2013.07.003.