
Download
ORIGINAL ARTICLE
Stressful life events, psychiatric comorbidities and serum neuromediator levels in patients with chronic spontaneous urticaria treated with omalizumab
Akdaş Elçina*, Gülekon Aylab, Bulut Tuba Saadet Devecic, Gülbahar Özlemc, Öztürk Murata, Başaran Ahmet Selimd, Coşar Behçetd
aDepartment of Dermatovenereology, Van Training and Research Hospital, Health Sciences University, Van, Turkey
bDepartment of Dermatovenereology, Faculty of Medicine, Gazi University, Ankara, Turkey
cDepartment of Biochemistry, Faculty of Medicine, Gazi University, Ankara, Turkey
dDepartment of Psychodermatology, Faculty of Medicine, Gazi University, Ankara, Turkey
Abstract
Introduction: Many chronic spontaneous urticaria (CSU) patients have highly stressful life events and exhibit psychiatric comorbidities. Emotional stress can cause or exacerbate urticaria symptoms by causing mast cell degranulation via neuromediators.
Objectives: To investigate the frequency of stressful life events and compare psychiatric comorbidities and serum neuromediator levels in patients with CSU who responded to omalizumab with healthy controls.
Methods: In this cross-sectional study, we included 42 patients with CSU who received at least 6 months of omalizumab treatment and a control group of 42 healthy controls. Stressful life events were evaluated with the Life Events Checklist for DSM-5 (LEC-5). The Depression Anxiety Stress Scale-42 (DASS-42) was used to evaluate depression, anxiety and stress levels. Serum nerve growth factor (NGF), calcitonin gene-related peptide (CGRP) and substance P (SP) levels were measured using the enzyme-linked immunosorbent assay (ELISA) technique.
Results: Twenty-six (62%) patients reported at least one stressful life event a median of 3.5 months before the onset of CSU. There were no significant differences in all three variables in the DASS subscales between the patient and control groups. Serum NGF levels were found to be significantly lower in patients with CSU (p <0.001), whereas CGRP levels were found to be significantly higher (p <0.001). There was no significant difference for SP.
Conclusions: The psychological status of patients with CSU who benefited from omalizumab was similar to that of healthy controls. Omalizumab may affect stress-related neuromediator levels.
Key words: spontaneous urticaria, omalizumab, stress, psychopathology, neuromediators
*Corresponding author: Dr. Elçin Akdaş, Department of Dermatovenereology, Van Training and Research Hospital, Health Sciences University, Van, Turkey. Email address: [email protected]
Received 11 October 2023; Accepted 29 January 2024; Available online 1 May 2024
Copyright: Akdaş E, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Chronic spontaneous urticaria (CSU) is a common disease in the community associated with a high disease burden on patients and the health system, including prolonged illness, frequent emergency and outpatient visits, sleep difficulties, and detrimental effects on work performance and social interactions.1 Autoimmunity mediated by pathogenic autoantibodies is involved in the pathogenesis of the disease in about half of the cases, but the underlying pathomechanism could not be determined in the others.2
Omalizumab effectively improves symptoms in a significant proportion of patients with CSU, but its mechanism of action in CSU has not been fully elucidated.3,4 Our experiences and evidence from previous studies have shown that in the significant proportion of patients who responded to omalizumab, it is unlikely to discontinue treatment for several years.5,6
There are observations that patients with CSU often experience unusual emotional stress before disease onset and report symptoms that are worsened by stress. It has also been reported that many patients with CSU exhibit a variety of psychiatric disorders, most commonly anxiety, depression and perceived stress.1 A recent meta--analysis of 25 studies revealed that almost one out of three patients with CSU has at least one underlying psychiatric disorder.7 The authors suggested that a ‘brain-skin’ link with local neuro-immune endocrine circuits may underlie the pathogenesis of stress-induced or exuberated allergic and inflammatory skin diseases.7,8 Many observations on the effects of stress on the neuroendocrine and immune systems in psoriasis, atopic dermatitis and prurigo nodularis support this theory.9–11 In this model, it has been suggested that emotional stress activates a hierarchical cascade of events which includes various neuronal mediators, such as nerve growth factor (NGF), calcitonin gene-related peptide (CGRP) and substance P (SP).8,12,13
The skin is highly innervated by numerous nerve fibre subpopulations originating from the dorsal root ganglia, where neuropeptides are produced and stored. Mast cells are located perivascular close to the peptidergic C fibres in the upper dermis, an ideal location for sensory nerve stimulation.12 Emotional stress and various external stimuli result in the depolarising of sensory nerve fibres, and subsequently release numerous mediators, including neuropeptides, neurotrophins and hormones stored in the cytoplasmic vesicles of nociceptive neurons from the axon terminals to the stimulated area antidromically.12,13 This mechanism allows a rapid response to occur long before the immune system is stimulated.13 Neuropeptides released by stimulation of sensory fibres lead to mast cell degranulation. In turn, itch-related mediators including histamine, tryptase and NGF released from mast cells, also stimulate peptidergic C fibres, which store proinflammatory neuropeptides such as CGRP and SP. This bidirectional positive feedback between mast cells and sensory fibres exacerbates mast cell-mediated neurogenic inflammation and pruritus.8,12,13
Skin mast cells are considered the primary effector cells in urticaria. In addition to IgE-dependent degranulation, there is evidence that many signals can target skin mast cells through IgE-independent mechanisms by various receptors, including G-protein coupled and complement receptors.4,14,15 It was reported that emotional stress may cause urticaria symptoms by increasing mast cell degranulation via G-protein coupled receptors in a neuropeptide-dependent manner.14,15
The aim of our cross-sectional, case-controlled study was to assess the role of psychiatric disorders in CSU, and the effect of omalizumab on NGF, CGRP and SP levels in patients who responded to omalizumab, apart from its anti-IgE effect. We also investigated stressful life events that occurred before the onset of illness in CSU patients.
Materials and Methods
Study population
This cross-sectional, case-controlled study was performed between August 2021 and November 2021 at the Department of Dermatology, Gazi University Faculty of Medicine Research Hospital which is a tertiary hospital in Ankara, Turkey. Patients who had been followed up in our specialised urticaria outpatient clinic and had received at least 6 months of omalizumab (300 mg/month) for CSU were included in the study.
In the patient group, age, gender, concomitant angioedema, concurrent chronic inducible urticaria, duration of CSU, duration of omalizumab, 7-day urticaria activity score (UAS7) and urticaria control test (UCT) scores were recorded.
We excluded individuals with any previous inflammatory or allergic skin disease history, a diagnosed psychiatric disorder, and the use of psychotropic substances within 6 months, marked cognitive impairment, or who received glucocorticoid therapy for at least 1 month. All participants provided informed consent. The study was approved by the Institutional Ethics Committee (Approval number: 07.2020.599).
Mental assessment and psychometric instruments
The levels of depression, anxiety and stress were assessed with the Depression Anxiety Stress Scale-42 (DASS-42), which is a self-administered questionnaire designed to measure the magnitude of three negative emotional states.16 DASS is a 42-item questionnaire consisting of three subscales, each containing 14 items scored on a four-point scale ranging from 0 (did not apply to me at all) to 3 (applied to me very much), measuring the extent to which each item was experienced over the previous week. The DASS depression focuses on reports of low mood, motivation and self-esteem; DASS-anxiety on physiological arousal, perceived panic and fear; and DASS-stress on tension and irritability.
Stressful life events were assessed with the Life Events Checklist for DSM-5 (LEC-5), a self-report measure developed to screen for lifetime traumatic events.17 The instrument assesses exposure to 16 different adverse life events that may potentially result in post-traumatic stress disorder or distress and includes one additional item considering any other extraordinarily stressful event not captured in the first 16 items.
Measurement of NGF, CGRP and SP levels
In addition to routine examinations, 5 mL of blood was taken from the patient and control group into the coagulation activator tube and centrifuged at 3000 rpm for 10 min at room temperature. In the next step, the serum was separated, transferred to the Eppendorf tube, isolated and stored at -80°C until the test time. After all sera were collected, serum NGF, CGRP and SP levels were measured using an enzyme-linked immunosorbent assay (ELISA) kit (Elabscience Biotechnology Inc., 14780 Memorial Drive, Suite 216, Houston, Texas 77079 USA) according to manufacturer’s instructions.
Statistical analysis
Statistical analysis was performed using SPSS 27.0 (SPSS Inc., Chicago, USA). Baseline characteristics of cases and controls were analysed using descriptive statistics. We assessed the comparisons between groups for the categorical variables using the Chi-square test. The normality of continuous data was assessed by the Kolmogrov–Smirnov test. A comparison of the various parameters between patients and controls was performed by the independent sample t-test for parametric data. The Mann–Whitney U-test was used for paired group comparison of numerical variables when the variables were not normally distributed. Correlation analysis was performed using the Spearman correlation test. The data were described as mean (standard deviation [SD]) or median (interquartile range [IQR]), as appropriate. The level of statistical significance was set at p <0.05.
Results
A total of 42 CSU patients and 42 healthy controls (as a control group) were included in this cross-sectional study during the 4 months of enrollment. The demographic features and disease characteristics of the study groups are summarised in Table 1. Of 42 patients with CSU, 29 (69%) had concomitant angioedema and 26 (62%) had concurrent inducable urticaria. The median duration of omalizumab treatment was 21.5 months (IQR, 6–65). The median UAS7 and UCT scores were 6 (IQR, 2–15) and 17 (IQR, 16–18), respectively.
Table 1. The demographics and disease characteristics of the study groups.
| CSU (n = 42) | Control (n = 42) | p | |
|---|---|---|---|
| Age, year, mean± SD (min–max) | 42±8 (23–56) | 39±10 (21–65) | 0.201 |
| Female, n (%) | 32 (76) | 29 (69) | 0.463 |
| Concomitant angioedema, n (%) | 29 (69) | - | - |
| Concurrent inducable urticaria, n (%) | 26 (62) | - | - |
| Disease duration, month, median (IQR) | 44 (10–362) | - | - |
| Treatment duration with omalizumab, median (IQR) | 21.5 (6–65) | - | - |
| UAS7, median (IQR) | 6 (2–15) | - | - |
| UCT, median (IQR) | 13 (12–14.25) | - | - |
| Stressful life events prior to disease, n (%) | 26 (62) | - | - |
CSU, chronic spontaneous urticaria; UAS7, weekly urticaria activity score; UCT, urticaria activity score; SD, standard deviation; IQR, interquartile range.
Among the 42 patients, 26 (62%) noted at least one stressful life event preceding the exacerbation of CSU, and 32 (74%) reported that their urticaria symptoms were exacerbated by stress. The median duration between the event and CSU onset was 3.5 months (range, 0 and 4 months).
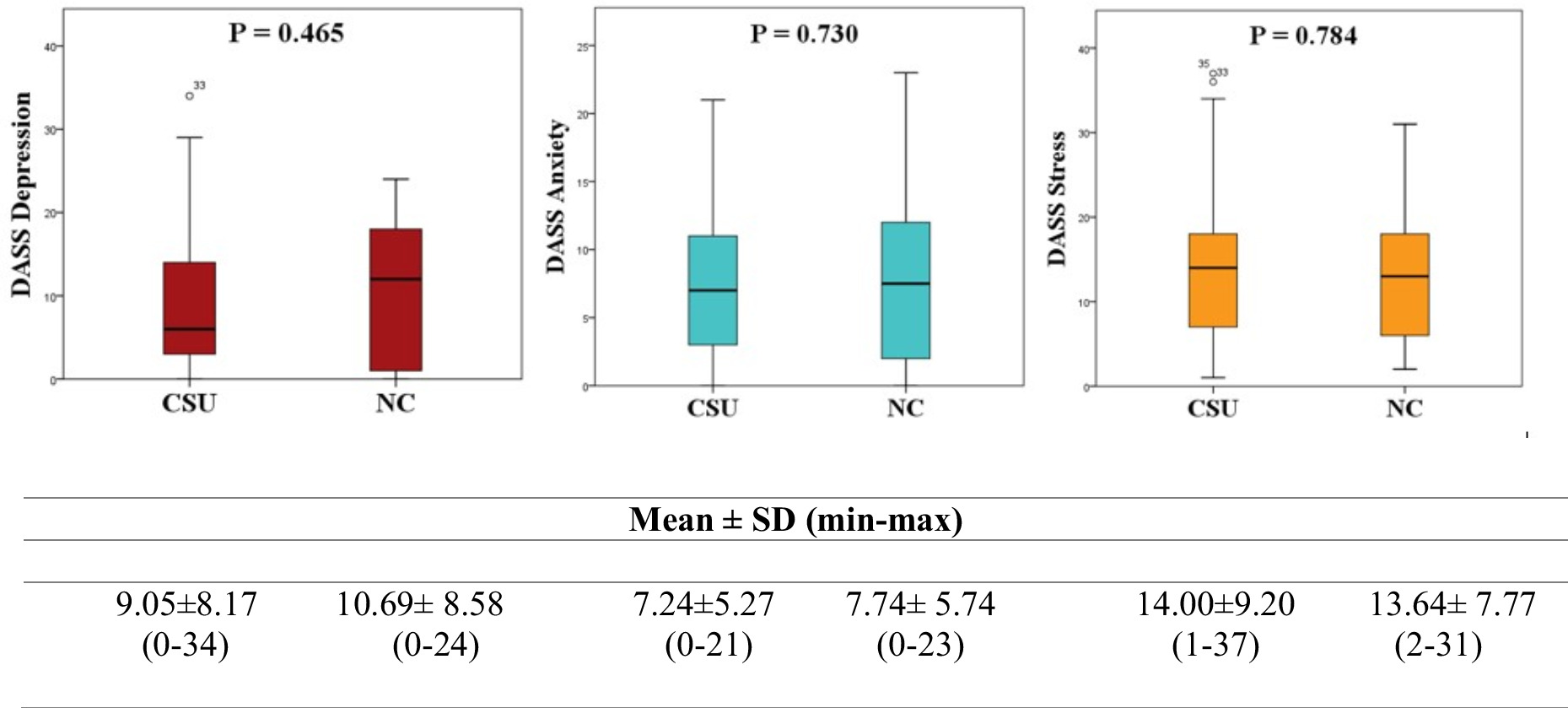
There were no significant differences in all three variables in the DASS subscales between the patient and control groups (depression: p = 0.465; anxiety: p = 0.730; stress: p = 0.784) (Figure 1).
Figure 1 Comparison of depression, anxiety and stress levels between CSU patients and normal controls. p values were obtained by the independent sample t-test. DASS, Depression Anxiety Stress Scale; SD, standard deviation; CSU, chronic spontaneous urticaria; NC, normal healthy controls.
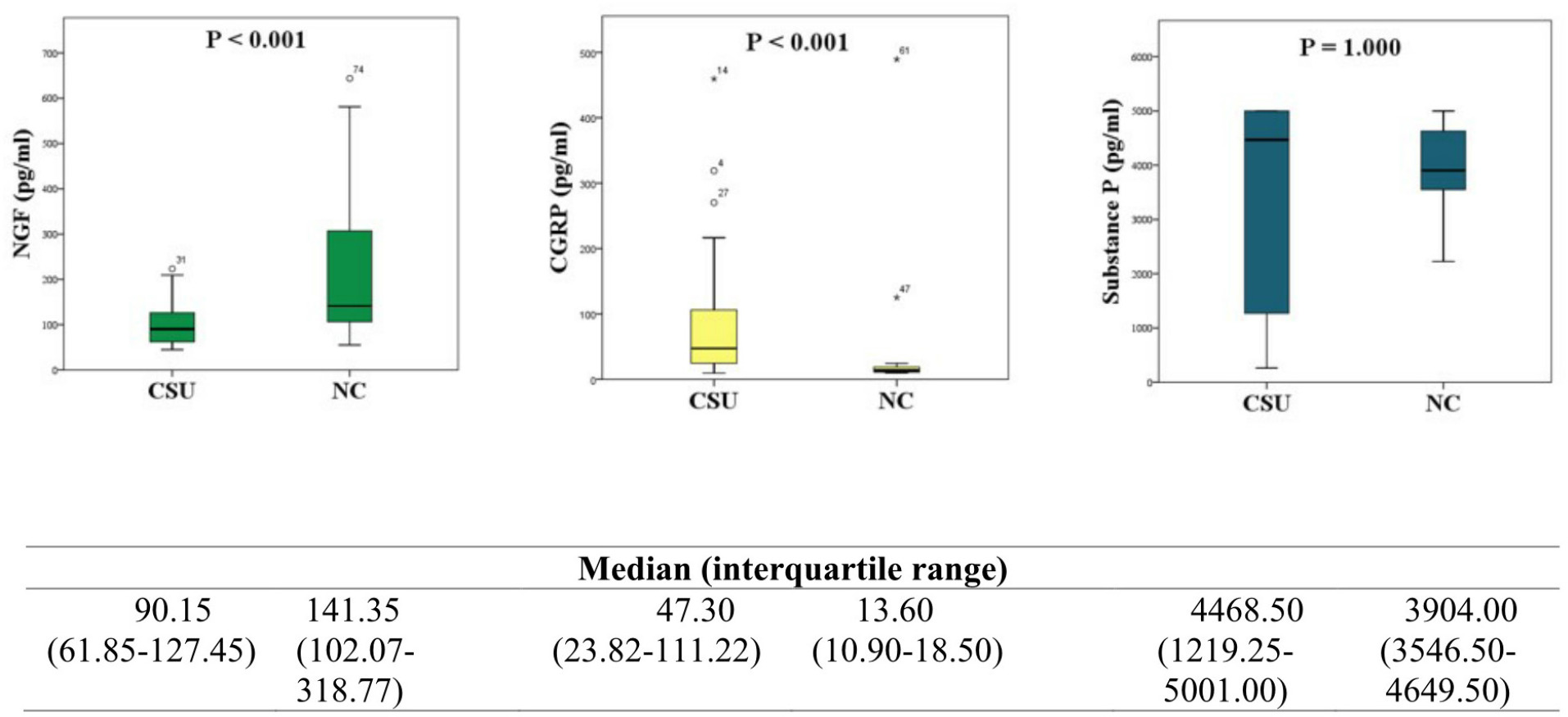
Serum NGF levels were significantly lower in the CSU group compared with the controls (median [interquartile range], 90.15 pg/mL [61.85–127.45], p <0.001), whereas CGRP levels were found to be significantly higher (47.30 pg/mL [23.82–111.22], p <0.001). There was no significant difference in SP levels between the two groups (Figure 2).
Figure 2 Comparison of NGF, CGRP and SP levels between CSU patients and normal controls. p values were obtained by the Mann–Whitney U-test. NGF, nerve growth factor; CGRP, calcitonin gene-related peptide; substance P, SP; IQR, interquartile range; CSU, chronic spontaneous urticaria; NC, normal healthy controls.
We also analysed the relationship between UCT and UAS7 scores and DASS42 subscales scores and levels of three neuromediators. Correlation analyses revealed that in CSU patients, UAS7 scores showed a significant positive correlation with DASS42 scale results for ‘anxiety’ (r = 0.448; p = 0.003) and a trend towards ‘depression’ (r = 0.285; p = 0.068). Moreover, UCT scores showed a significant negative correlation with the DASS42 scale results for ‘anxiety’ (r = -0.399; p = 0.009) and a trend towards ‘depression’ (r = -0.277; p = 0.076). Stress scores did not correlate with UAS7 or UCT scores (p>0.05). It was revealed that CGRP levels among neuropeptides showed a positive correlation with UAS7 scores (r = 0.326; p = 0.035) and a negative correlation with UCT scores (r = -0.331; p = 0.032). No correlation was shown for substance P and NGF (Table 2).
Table 2. Spearman’s correlation between UAS7 scores, UCT scores and study parameters.
| UAS7 | UCT | |||
|---|---|---|---|---|
| r | p | r | p | |
| NGF (pg/mL) | -0.022 | 0.892 | 0.004 | 0.979 |
| CGRP (pg/mL) | 0.326 | 0.035 | -0.331 | 0.032 |
| SP (pg/mL) | 0.050 | 0.752 | -0.101 | 0.526 |
| DASS-Depression | 0.285 | 0.068 | -0.277 | 0.076 |
| DASS-Anxiety | 0.448 | 0.003 | -0.399 | 0.009 |
| DASS-Stress | 0.128 | 0.418 | -0.220 | 0.162 |
UAS7, weekly urticaria activity score; UCT, urticaria activity score; DASS, Depression Anxiety Stress Scale; NGF, nerve growth factor; CGRP, calcitonin gene-related peptide; substance P, SP.
Discussion
In this study, we found that CSU patients who achieved symptomatic relief with omalizumab treatment had similar depression, anxiety and stress levels as that of healthy controls. These findings contradict the studies reporting a higher incidence of psychiatric comorbidities in patients with CSU,7 but support some recent studies showing that omalizumab treatment improves psychiatric parameters in patients with CSU.18–20 In their study, Diluvio et al. revealed that CSU patients demonstrated markedly reduced psychological health subscale scores compared with controls. They showed that after 6 months of treatment with omalizumab, 71% of subjects who had obtained a borderline or abnormal score for depression received a normal score and 60% of subjects with a previous abnormal anxiety score achieved a normal score for anxiety.19 Similarly, Patella et al. observed that all the psychological scores (PSS for perceived stress, HADS-A for anxiety and HADS-D for depression) were improved after 24 weeks of treatment with omalizumab in refractory CSU patients.20 A recent study with asthma patients has also shown that omalizumab reduced symptoms of depression and stress in these patients as well.21
In this study, almost two-third (62%) of CSU patients were found to have experienced a stressful life event a median of three and a half months before the onset of urticaria. These results concord with previous studies, which showed that patients with CSU had significantly more life events in the 6 months before the disease onset.22–24
A recent meta-analysis reported no relationship between psychiatric illness and the severity of CSU,7 however, we found anxiety scores positively correlated with UAS7 scores and negatively correlated with UCT scores in patients with CSU. Moreover, there was a similar trend for depression, although it was not statistically significant. Our findings align with a study by Tat et al., who reported a significant positive correlation between UAS and anxiety and depression scores in patients with chronic urticaria.25
In their recent systematic review, Konstantinou et al.26 considered that stress-induced imbalance or irregularity of the neuro-immune-cutaneous circuit may contribute to the pathophysiology of chronic urticaria. Emotional stress increases neurogenic inflammation by both modulating the hypothalamic-pituitary-adrenal axis in the brain and skin and increasing neuromediator levels. As a result, many chronic inflammatory skin diseases may emerge and exacerbate.12–14 A number of studies have shown that in numerous inflammatory and autoimmune diseases, including urticaria, tissue and serum NGF levels increase compared with healthy controls.14,27,28
We found significantly lower levels of serum NGF in patients with CSU compared to controls. Bonini et al., in their study to compare serum NGF levels between patients with asthma and/or rhinoconjunctivitis and/or urticaria--angioedema and healthy controls, observed that serum NGF levels were higher in allergic diseases. They also showed a positive correlation between NGF levels and total IgE levels.29 In another study in which mouse and human in vitro cultured mast cells were activated by IgE, NGF secretion increased as measured by ELISA and RT-PCR was shown.30 Considering that omalizumab binds to free IgE in mast cells and inhibits IgE-mediated FcɛRI activation, these data reinforce that NGF release was decreased secondary to inhibition of IgE-mediated mast cell activation.
Nerve growth factor is an essential neuromediator for the survival of nociceptive neurons during development and neurogenic inflammation. Sensory nerve fibres in the skin end by branching towards areas with high NGF concentrations. Therefore, NGF determines the sensitivity threshold in the interactions between mast cells and nerve fibres, while a hyperreactive state occurs in pathophysiological conditions, resulting in increased skin sensitivity in the local environment to neurogenic flare, itch and pain.14 Taken together, omalizumab may increase the threshold of sensitivity of sensory nerve fibres to stress and other external stimuli by decreasing NGF levels.
Nerve growth factor also exacerbates neurogenic inflammation by causing increased expression of TRPV1 in nerve fibres, followed by the release of SP and CGRP, thus creating a vicious cytokine ‘pro-itch’ cycle.13 Joachim et al. showed that both stress exposure and injection of NGF up-regulated the percentage of SP+ or CGRP+ sensory neurons in murine skin.8 Substance P and CGRP are classical neuropeptides that mediate vascular effects by acting directly on vascular endothelial cells and smooth muscle cells. CGRP is one of the most potent microvascular vasodilator mediators known to contribute to most neurogenic vasodilation. Substance P increases vascular permeability with subsequent plasma extravasation and oedema.13 Some evidence has recently been presented that especially SP and CGRP neuropeptides may play a vital role in the pathophysiology of urticaria.14,26 In a series of studies by Kimata et al.,31–33 it has been shown that the stress of playing video games, listening to cell phones and exposure to road traffic increases allergen-induced wheal responses in parallel with increased plasma levels of SP, VIP and NGF. Borici-Mazi et al., in their study to compare the cutaneous responses to SP and CGRP in patients with chronic urticaria with healthy adults, observed the skin of patients with chronic urticaria increased sensitivity to the neuropeptide SP and CGRP.34 In another study, lesional skin in CSU was found to contain significantly more CGRP than non-lesional skin.35
We found that serum CGRP levels were markedly higher in the patient group compared with healthy controls, whereas there was no difference in SP levels. In parallel with our findings, Tedeschi et al.36 reported that SP levels were not found to be higher in CSU patients than in controls, whereas several studies showed that circulating SP levels in CSU patients were higher than in healthy controls.37–39 Despite several studies evaluating CGRP levels and their effects on the skin, little is known about circulating CGRP levels in patients with CSU. In a study conducted by Başak et al., in which they compared the neuropeptide levels of patients with chronic urticaria and healthy controls, it was found that no difference was found between CGRP levels while SP levels were significantly higher in patients with chronic urticaria compared to control.39 Another study by the same author reported that antihistamine treatment did not affect serum SP levels but increased CGRP levels in chronic urticaria.40 We obtained similar results in our study involving patients under omalizumab treatment. It has been reported that neuropeptides activate skin mast cells via G-protein-coupled receptors in a neuropeptide-dependent manner, not via FcɛRI receptors in an IgE-dependent manner.14,15 These findings indicate that omalizumab may affect the levels of neuropeptides which are closely related to stress, apart from the decrease in free IgE and FcɛRI levels on mast and basophil cells, which is the known mechanism of action in urticaria.
Limitations
The limitations of our study include that since our study was a cross-sectional study, the depression, anxiety and stress levels of the patients before omalizumab could not be shown. Another limitation is that serum neuromediator levels had yet to be measured before omalizumab, as the literature, which suggested neuropeptides induce mast cells in an IgE-independent manner14,15 was taken into account in our study. However, our study findings suggested that omalizumab may affect neuronal mediator levels as well as prevents IgE-mediated mast cell activation. Investigating the effects of omalizumab on neuropeptide and neurotrophin levels in CSU might also be another interesting subject for further studies.
Conclusions
We found that the depression, anxiety and stress levels of patients with CSU who benefited from omalizumab and received treatment for more than 6 months were similar to those of the healthy subjects. However, the fact that two-third of the patients reported a stressful life event before the disease suggests that stress may play a role in the onset and exacerbation of urticaria in suspected individuals. However, the fact that two-third of the patients reported a stressful life event before the disease suggests that stress may play a key role in the onset and exacerbation of urticaria in suspected individuals. The known action of omalizumab, reducing free IgE levels and down--regulating FcɛRI receptors, does not explain all of its effects in CSU. The striking differences in CSU patients treated with omalizumab for NGF and CGRP in our study compared to healthy controls suggest that omalizumab affects neuromediator levels associated with stress and neurogenic inflammation. Further prospective studies are needed to better understand the effect of omalizumab on psychiatric comorbidities and stress-related neuromediators in CSU and to confirm our results.
Authorship
All authors have contributed significantly to this publication.
Financial support and sponsorship
None.
Conflict of interest
There are no conflicts of interest.
REFERENCES
1. Maurer M, Weller K, Bindslev-Jensen C, Giménez-Arnau A, Bousquet PJ, Bousquet J, et al. Unmet clinical needs in chronic spontaneous urticaria. A GA2LEN task force report. Allergy. 2011;66(3):317–30. 10.1111/j.1398-9995.2010.02496.x
2. Kaplan A, Greaves M. Pathogenesis of chronic urticaria. Clin Exp Allergy. 2009;39(6):777–87. 10.1111/j.1365-2222.2009.03256.x
3. Türk M, Carneiro-Leão L, Kolkhir P, Bonnekoh H, Buttgereit T, Maurer M. How to treat patients with chronic spontaneous urticaria with omalizumab: Questions and answers. J Allergy Clin Immunol Pract. 2020;8(1):113–24. 10.1016/j.jaip.2019.07.021
4. Maurer M, Eyerich K, Eyerich S, Ferrer M, Gutermuth J, Hartmann K, et al. Urticaria: Collegium internationale allergologicum (CIA) update 2020. Int Arch Allergy Immunol. 2020;181(5):321–33. 10.1159/000507218
5. Bernstein JA, Kavati A, Tharp MD, Ortiz B, MacDonald K, Denhaerynck K, et al. Effectiveness of omalizumab in adolescent and adult patients with chronic idiopathic/spontaneous urticaria: A systematic review of ‘real-world’ evidence. Expert Opin Biol Ther. 2018;18(4):425–48. 10.1080/14712598.2018.1438406
6. Akdaş E, Adışen E, Öztaş MO, Aksakal AB, İlter N, Gülekon A. Real-life clinical practice with omalizumab in 134 patients with refractory chronic spontaneous urticaria: A single-center experience. An Bras Dermatol. 2023;98(2):240–2. 10.1016/j.abd.2022.06.003
7. Konstantinou GN, Konstantinou GN. Psychiatric comorbidity in chronic urticaria patients: A systematic review and meta-analysis. Clin Transl Allergy. 2019;9(1):1–12. 10.1186/s13601-019-0278-3
8. Joachim RA, Kuhlmei A, Dinh Q, Handjiski B, Fischer T, Peters EM, et al. Neuronal plasticity of the “brain–skin connection”: Stress-triggered up-regulation of neuropeptides in dorsal root ganglia and skin via nerve growth factor-dependent pathways. J Mol Med. 2007;85(12):1369–78. 10.1007/s00109-007-0236-8
9. Zhang Y, Zhang H, Jiang B, Tong X, Yan S, Lu J. Current views on neuropeptides in atopic dermatitis. Exp Dermatol. 2021;30(11):1588–97. 10.1111/exd.14382
10. Ayasse MT, Buddenkotte J, Alam M, Steinhoff M. Role of neuroimmune circuits and pruritus in psoriasis. Exp Dermatol. 2020;29(4):414–26. 10.1111/exd.14071
11. Williams KA, Roh YS, Brown I, Sutaria N, Bakhshi P, Choi J, et al. Pathophysiology, diagnosis, and pharmacological treatment of prurigo nodularis. Expert Rev Clin Pharmacol. 2021;14(1):67–77. 10.1080/17512433.2021.1852080
12. Arck PC, Slominski A, Theoharides TC, Peters EM, Paus R. Neuroimmunology of stress: Skin takes center stage. J Invest Dermatol. 2006;126(8):1697–704. 10.1038/sj.jid.5700104
13. Choi JE, Di Nardo A. Skin neurogenic inflammation. Semin Immunopathol. 2018;40(3):249–59. 10.1007/s00281-018-0675-z
14. Church MK, Kolkhir P, Metz M, Maurer M. The role and relevance of mast cells in urticaria. Immunol Rev. 2018;282(1):232–47. 10.1111/imr.12632
15. Babina M, Guhl S, Artuc M, Zuberbier T. Allergic FcɛRI-and pseudo-allergic MRGPRX 2-triggered mast cell activation routes are independent and inversely regulated by SCF. Allergy. 2018;73(1):256-60. 10.1111/all.13301
16. Bilgel NG, Bayram N. Turkish version of the depression anxiety stress scale (DASS-42): Psychometric properties. Noro Psikiyatr Ars. 2010;48(3):118–26. 10.4274/npa.5344
17. Boysan M, Guzel Ozdemir P, Ozdemir O, Selvi Y, Yilmaz E, Kaya N. Psychometric properties of the Turkish version of the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders, (PCL-5). Psychiatry Clin Psychopharmacol. 2017;27(3):300–10. 10.1080/24750573.2017.1342769
18. Can PK, Etikan P, Degirmentepe EN, Kocaturk E. Depression scores change significantly after omalizumab treatment in patients with chronic spontaneous urticaria. Asian Pac J Allergy Immunol. 2021;10 (Online ahead of print). 10.12932/AP-180920-0965
19. Diluvio L, Piccolo A, Marasco F, Vollono L, Lanna C, Chiaramonte B, et al. Improving of psychological status and inflammatory biomarkers during omalizumab for chronic spontaneous urticaria. Future Science OA. 2020;6(9):FSO618. 10.2144/fsoa-2020-0087
20. Patella V, Zunno R, Florio G, Palmieri M, Palmieri S, Brancaccio R. Omalizumab improves perceived stress, anxiety, and depression in chronic spontaneous urticaria. J Allergy Clin Immunol Pract. 2021;9(3):1402–4. 10.1016/j.jaip.2020.11.026
21. Uzer F, Ozbudak O. Benefits of omalizumab on anxiety and depression in patients with severe asthma. Casp J Intern Med.. 2018;9(3):228–31. 10.22088/cjim.9.3.228
22. Fava GA, Perini GI, Santonastaso P, Fornasa CV. Life events and psychological distress in dermatologic disorders: Psoriasis, chronic urticaria and fungal infections. Br J Med Psychol. 1980;53(3):277–82. 10.1111/j.2044-8341.1980.tb02551.x
23. Chung MC, Symons C, Gilliam J, Kaminski ER. Posttraumatic stress disorder, emotional suppression and psychiatric co-morbidity in patients with chronic idiopathic urticaria: A moderated mediation analysis. J Mental Health. 2018;27(5):442–9. 10.1080/09638237.2018.1437601
24. Yang H-Y, Sun C-C, Wu Y-C, Wang J-D. Stress, insomnia, and chronic idiopathic urticaria–A case-control study. J Formos Med Assoc. 2005;104(4):254–63. https://www.ncbi.nlm.nih.gov/pubmed/15909063
25. Tat TS. Higher levels of depression and anxiety in patients with chronic urticaria. Med Sci Monit. 2019;25:115. 10.12659/MSM.912362
26. Konstantinou GN, Konstantinou GN. Psychological stress and chronic urticaria: A neuro-immuno-cutaneous crosstalk. A systematic review of the existing evidence. Clin Ther. 2020;42(5):771–82. 10.1016/j.clinthera.2020.03.010
27. Skaper SD. Nerve growth factor: A neuroimmune crosstalk mediator for all seasons. Immunology. 2017;151(1):1–15. 10.1111/imm.12717
28. Peters EM, Liezmann C, Spatz K, Daniltchenko M, Joachim R, Gimenez-Rivera A, et al. Nerve growth factor partially recovers inflamed skin from stress-induced worsening in allergic inflammation. J Invest Dermatol. 2011;131(3):735–43. 10.1038/jid.2010.317
29. Bonini S, Lambiase A, Angelucci F, Magrini L, Manni L, Aloe L. Circulating nerve growth factor levels are increased in humans with allergic diseases and asthma. Proc Natl Acad Sci U S A . 1996;93(20):1095560. 10.1073/pnas.93.20.10955
30. Xiang Z, Nilsson G. IgE receptor-mediated release of nerve growth factor by mast cells. Clin Exp Allergy. 2000;30(10): 1379–86. 10.1046/j.1365-2222.2000.00906.x
31. Kimata H. Exposure to road traffic enhances allergic skin wheal responses and increases plasma neuropeptides and neurotrophins in patients with atopic eczema/dermatitis syndrome. Int J Hyg Environ Health. 2004;207(1):45–9. 10.1078/1438-4639-00261
32. Kimata H. Enhancement of allergic skin wheal responses by microwave radiation from mobile phones in patients with atopic eczema/dermatitis syndrome. Int Arch Allergy Immunol. 2002;129(4):348–50. 10.1159/000067592
33. Kimata H. Enhancement of allergic skin wheal responses in patients with atopic eczema/dermatitis syndrome by playing video games or by a frequently ringing mobile phone. Eur J Clin Invest. 2003;33(6):513–17. 10.1046/j.1365-2362.2003.01177.x
34. Borici-Mazi R, Kouridakis S, Kontou-Fili K. Cutaneous responses to substance P and calcitonin gene-related peptide in chronic urticaria: The effect of cetirizine and dimethindene. Allergy. 1999;54(1):46–56. 10.1034/j.1398-9995.1999.00726.x
35. Kay A, Ying S, Ardelean E, Mlynek A, Kita H, Clark P, et al. Calcitonin gene-related peptide and vascular endothelial growth factor are expressed in lesional but not uninvolved skin in chronic spontaneous urticaria. Clin Exp Allergy. 2014;44(8):1053–60. 10.1111/cea.12348
36. Tedeschi A, Lorini M, Asero R. No evidence of increased serum substance P levels in chronic urticaria patients with and without demonstrable circulating vasoactive factors. Clin Exp Dermatol. 2005;30(2):171–5. 10.1111/j.1365-2230.2005.01732.x
37. Zheng W, Wang J, Zhu W, Xu C, He S. Upregulated expression of substance P in basophils of the patients with chronic spontaneous urticaria: Induction of histamine release and basophil accumulation by substance P. Cell Biol Toxicol. 2016;32(3):217–28. 10.1007/s10565-016-9330-4
38. Metz M, Krull C, Hawro T, Saluja R, Groffik A, Stanger C, et al. Substance P is upregulated in the serum of patients with chronic spontaneous urticaria. J Invest Dermatol. 2014;134(11):2833–6. 10.1038/jid.2014.226
39. Basak P, Erturan I, Yuksel O, Kazanoglu O, Vural H. Evaluation of serum neuropeptide levels in patients with chronic urticaria. Indian J Dermatol Venereol Leprol. 2014;80(5):483. 10.4103/0378-6323.140345
40. Başak PY, Vural H, Kazanoglu OO, Erturan I, Buyukbayram HI. Effects of loratadine and cetirizine on serum levels of neuropeptides in patients with chronic urticaria. Int J Dermatol. 2014;53(12):1526–30. 10.1111/ijd.12590